

3D Printing Aids Acetabular Reconstruction in Complex Revision Hip Arthroplasty
- PMID: 28168060
- PMCID: PMC5259605
- DOI: 10.1155/2017/8925050
3D Printing Aids Acetabular Reconstruction in Complex Revision Hip Arthroplasty
Abstract
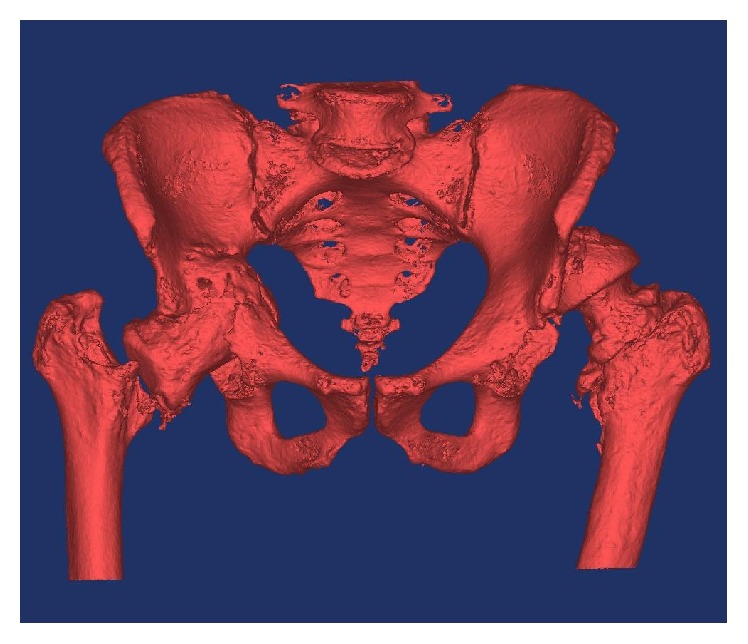
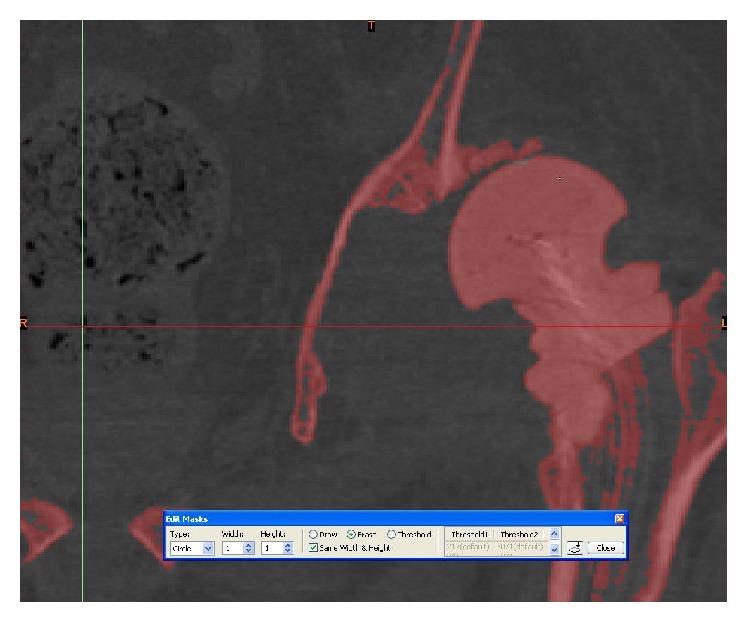
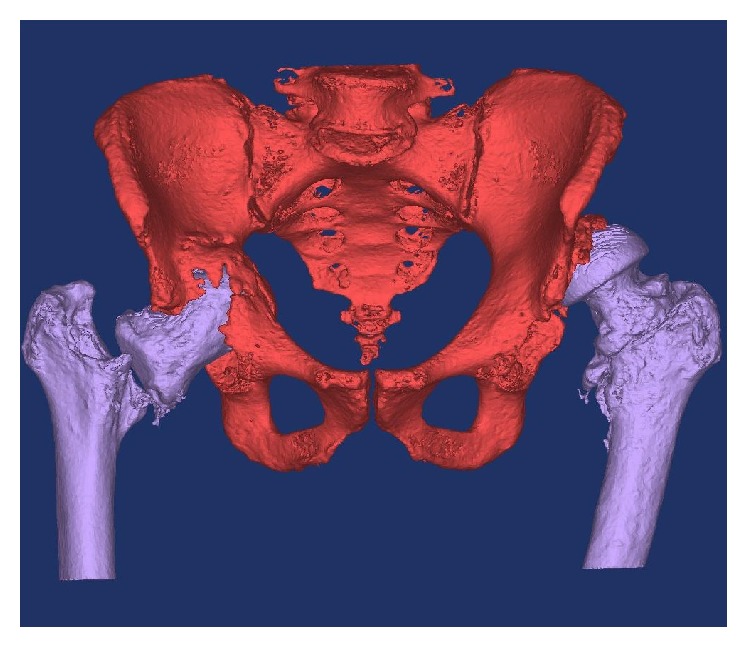
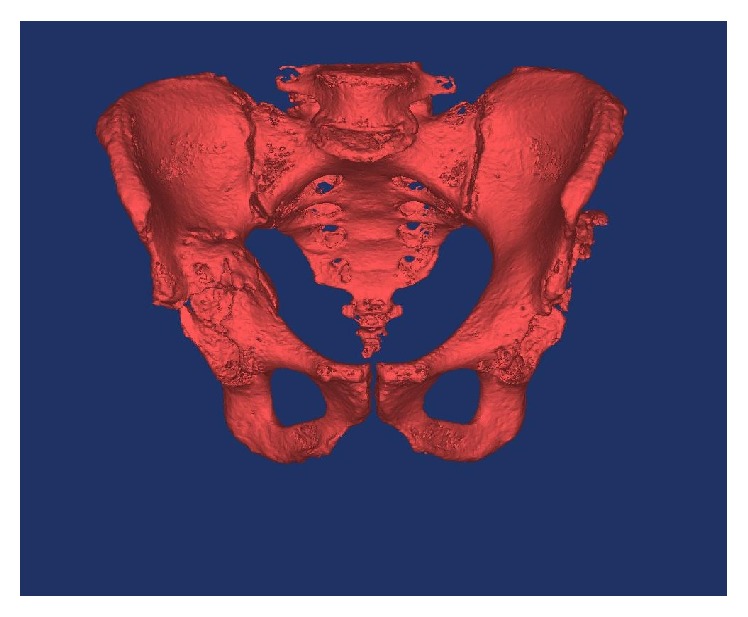
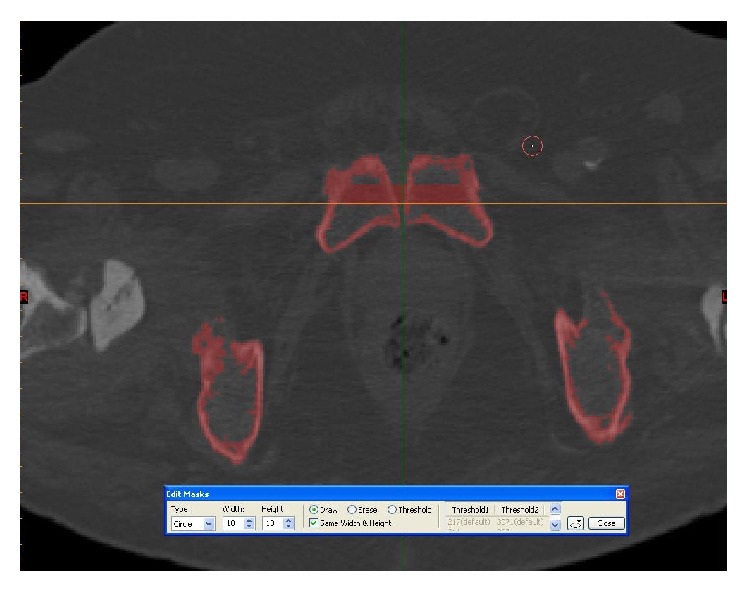
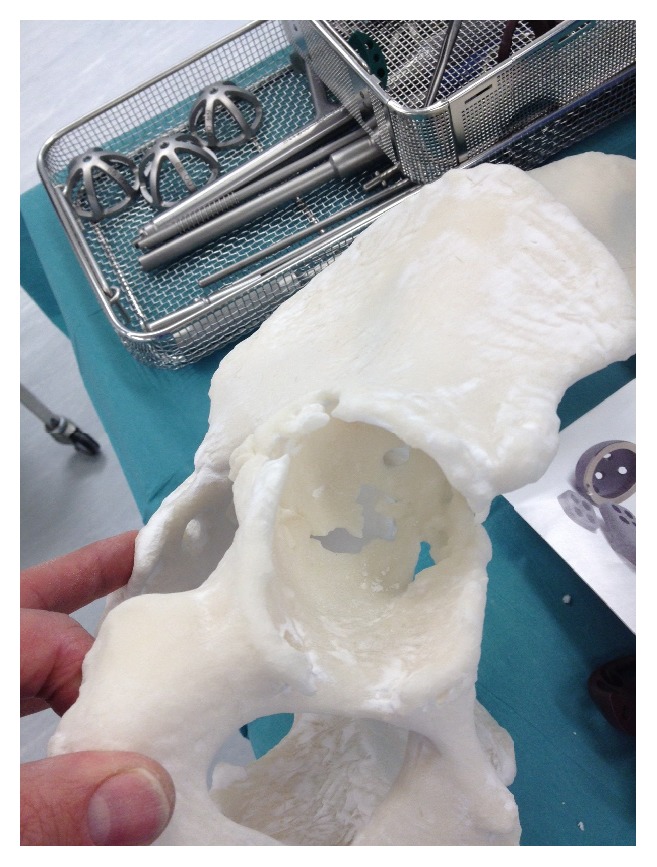
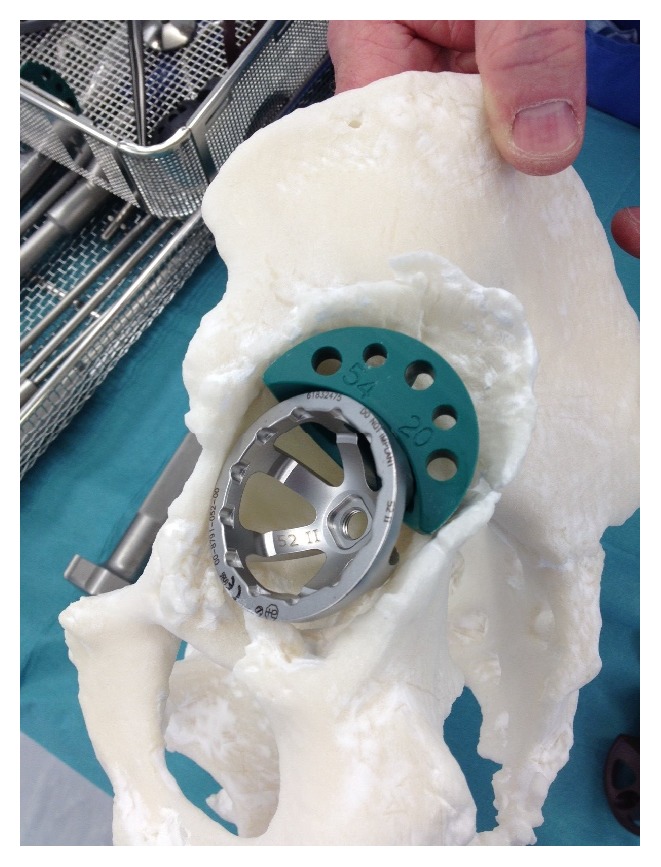
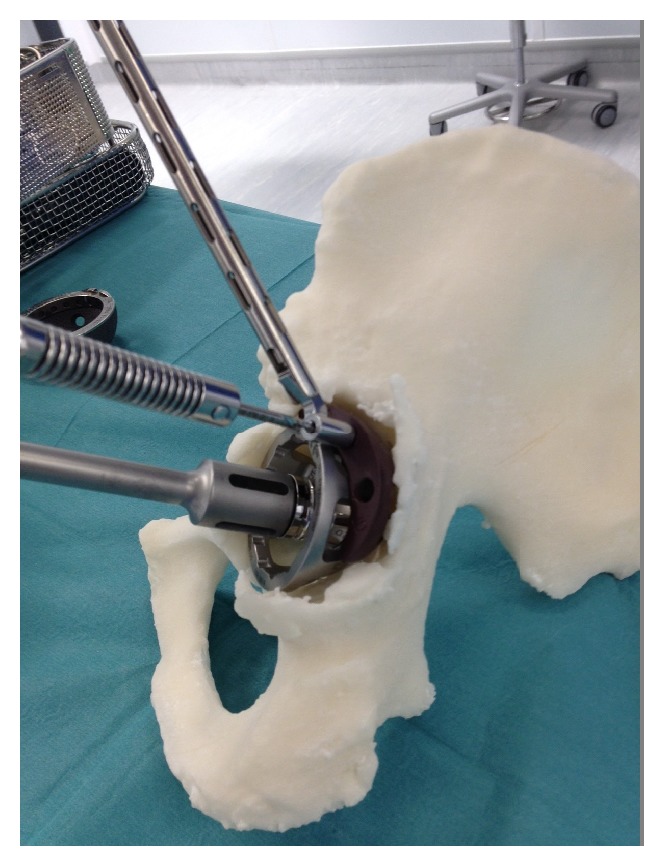
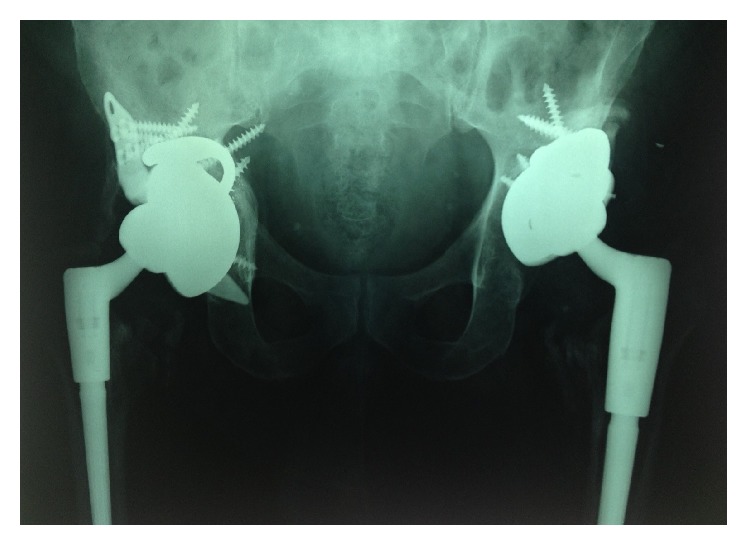
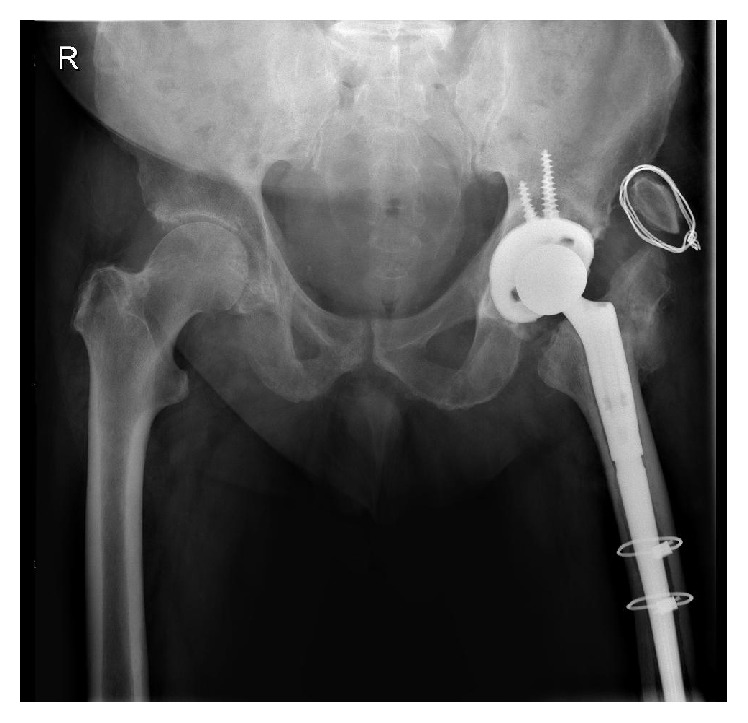
Revision hip arthroplasty requires comprehensive appreciation of abnormal bony anatomy. Advances in radiology and manufacturing technology have made three-dimensional (3D) representation of osseous anatomy obtainable, which provide visual and tactile feedback. Such life-size 3D models were manufactured from computed tomography scans of three hip joints in two patients. The first patient had undergone multiple previous hip arthroplasties for bilateral hip infections, resulting in right-sided pelvic discontinuity and a severe left-sided posterosuperior acetabular deficiency. The second patient had a first-stage revision for infection and recurrent dislocations. Specific metal reduction protocols were used to reduce artefact. The images were imported into Materialise MIMICS 14.12®. The models were manufactured using selective laser sintering. Accurate templating was performed preoperatively. Acetabular cup, augment, buttress, and cage sizes were trialled using the models, before being adjusted, and resterilised, enhancing the preoperative decision-making process. Screw trajectory simulation was carried out, reducing the risk of neurovascular injury. With 3D printing technology, complex pelvic deformities were better evaluated and treated with improved precision. Life-size models allowed accurate surgical simulation, thus improving anatomical appreciation and preoperative planning. The accuracy and cost-effectiveness of the technique should prove invaluable as a tool to aid clinical practice.
Conflict of interest statement
The authors declare that they have no competing interests.
Figures







Similar articles
-
Pre-operative planning and templating with 3-D printed models for complex primary and revision total hip arthroplasty.J Orthop. 2022 Sep 13;34:240-245. doi: 10.1016/j.jor.2022.09.004. eCollection 2022 Nov-Dec. J Orthop. 2022. PMID: 36120476 Free PMC article.
-
Three-dimensional printing for preoperative planning of total hip arthroplasty revision: case report.Skeletal Radiol. 2016 Oct;45(10):1431-5. doi: 10.1007/s00256-016-2444-1. Epub 2016 Aug 1. Skeletal Radiol. 2016. PMID: 27480617
-
Three-dimensional technology assisted trabecular metal cup and augments positioning in revision total hip arthroplasty with complex acetabular defects.J Orthop Surg Res. 2019 Dec 11;14(1):431. doi: 10.1186/s13018-019-1478-1. J Orthop Surg Res. 2019. PMID: 31829273 Free PMC article.
-
Acetabular reconstruction using porous metallic material in complex revision total hip arthroplasty: A systematic review.Orthop Traumatol Surg Res. 2019 Feb;105(1S):S53-S61. doi: 10.1016/j.otsr.2018.04.030. Epub 2018 Aug 20. Orthop Traumatol Surg Res. 2019. PMID: 30138711
-
Surgical applications of three-dimensional printing in the pelvis and acetabulum: from models and tools to implants.Unfallchirurg. 2019 Apr;122(4):278-285. doi: 10.1007/s00113-019-0626-8. Unfallchirurg. 2019. PMID: 30887060 Free PMC article. Review.
Cited by
-
Three-Dimensional Models in Planning of Revision Hip Arthroplasty with Complex Acetabular Defects.Indian J Orthop. 2018 Nov-Dec;52(6):625-630. doi: 10.4103/ortho.IJOrtho_556_16. Indian J Orthop. 2018. PMID: 30532303 Free PMC article.
-
Accuracy of Personalized Computed Tomographic 3D Templating for Acetabular Cup Placement in Revision Arthroplasty.Medicina (Kaunas). 2023 Sep 6;59(9):1608. doi: 10.3390/medicina59091608. Medicina (Kaunas). 2023. PMID: 37763727 Free PMC article.
-
Restoring Rotation Center in Total Hip Arthroplasty for Developmental Dysplasia of the Hip with the Assistance of Three Dimensional Printing Technology: A Pilot Study.Orthop Surg. 2022 Jan;14(1):119-128. doi: 10.1111/os.13183. Epub 2021 Dec 13. Orthop Surg. 2022. PMID: 34898037 Free PMC article.
-
Three-dimensional models of physeal fractures in the femur for the teaching of veterinary medicine.Acta Cir Bras. 2024 Aug 5;39:e395424. doi: 10.1590/acb395424. eCollection 2024. Acta Cir Bras. 2024. PMID: 39109784 Free PMC article.
-
Discussion on the possibility of multi-layer intelligent technologies to achieve the best recover of musculoskeletal injuries: Smart materials, variable structures, and intelligent therapeutic planning.Front Bioeng Biotechnol. 2022 Sep 30;10:1016598. doi: 10.3389/fbioe.2022.1016598. eCollection 2022. Front Bioeng Biotechnol. 2022. PMID: 36246357 Free PMC article. Review.
References
-
- Wroblewski B. M. Current trends in revision of total hip arthroplasty. International Orthopaedics. 1984;8(2):89–93. - PubMed
-
- Furnes O., Lie S. A., Espehaug B., Vollset S. E., Engesaeter L. B., Havelin L. I. Hip disease and the prognosis of total hip replacements. A review of 53,698 primary total hip replacements reported to the Norwegian Arthroplasty Register 1987–99. Journal of Bone and Joint Surgery B. 2001;83(4):579–586. doi: 10.1302/0301-620x.83b4.11223. - DOI - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources
