

Accuracy of iodine quantification using dual energy CT in latest generation dual source and dual layer CT
- PMID: 28168368
- PMCID: PMC5544802
- DOI: 10.1007/s00330-017-4752-9
Accuracy of iodine quantification using dual energy CT in latest generation dual source and dual layer CT
Abstract
Objective: To determine the accuracy of iodine quantification with dual energy computed tomography (DECT) in two high-end CT systems with different spectral imaging techniques.
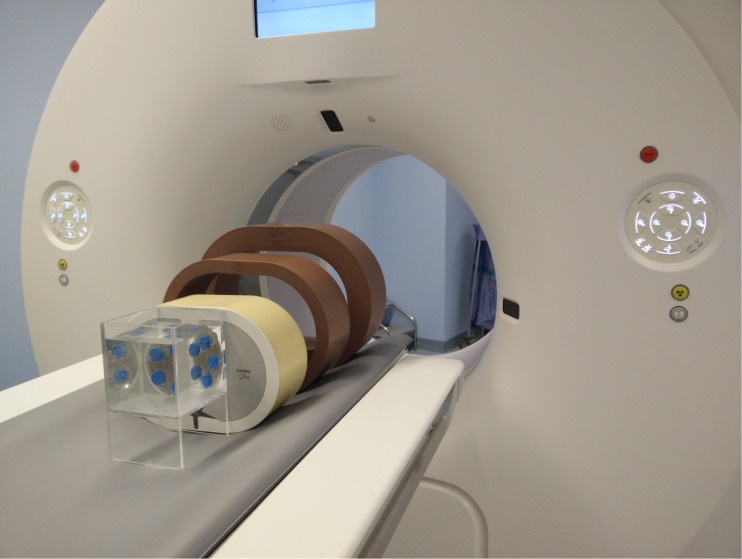
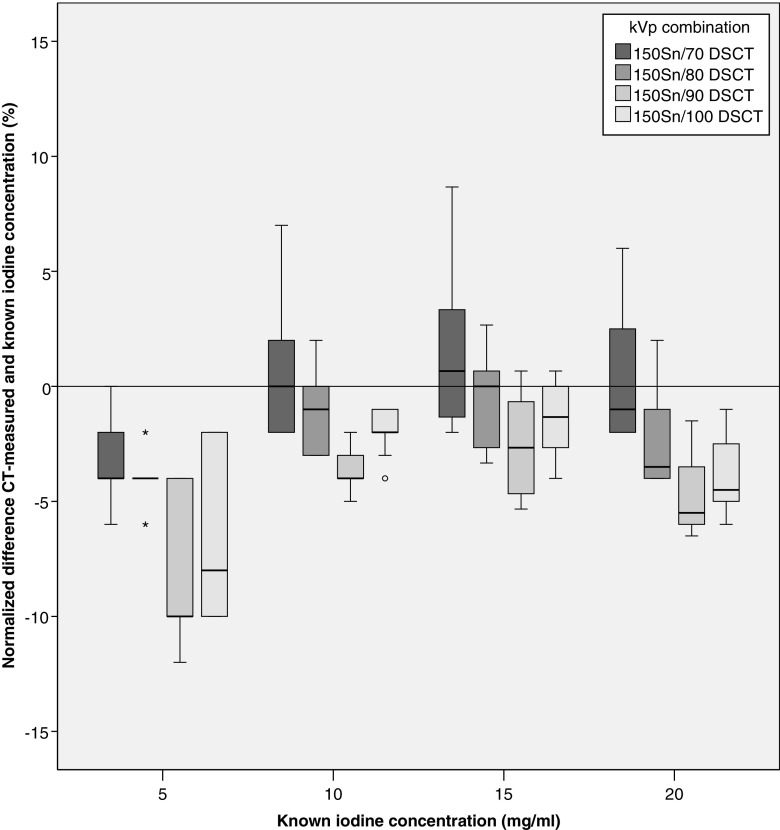
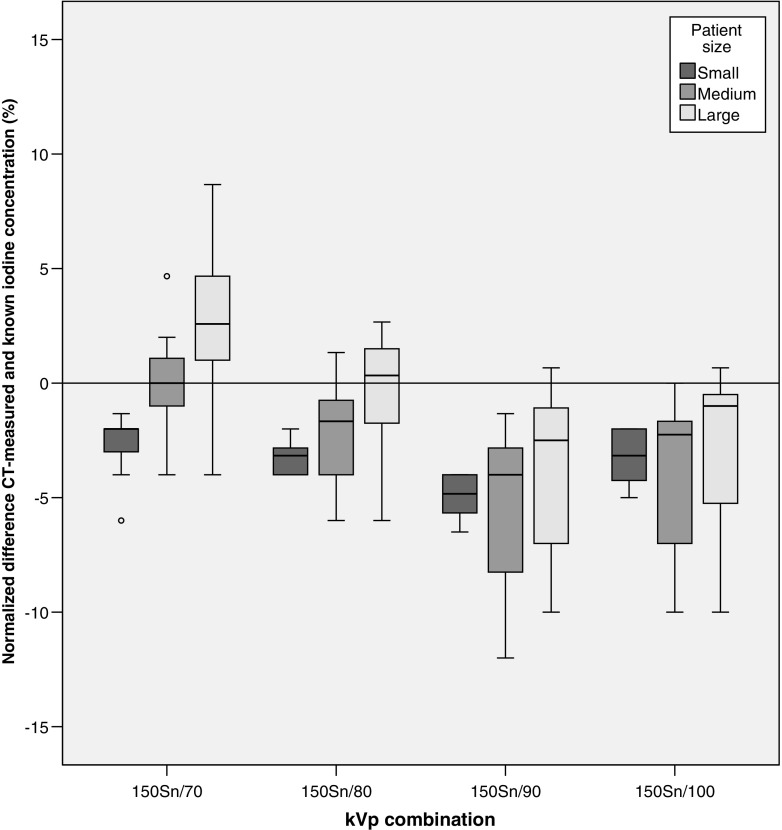
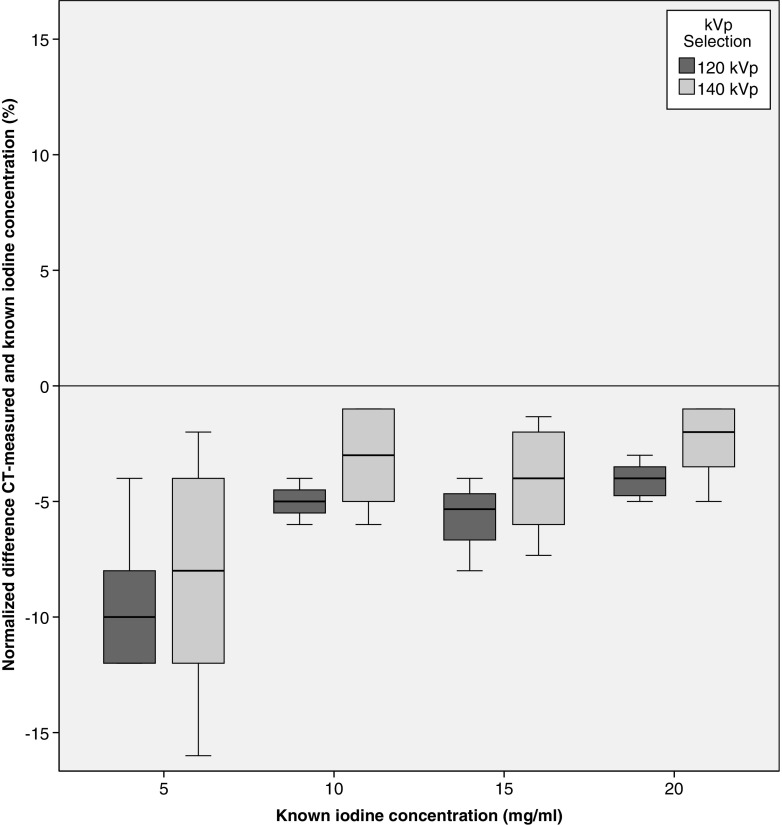
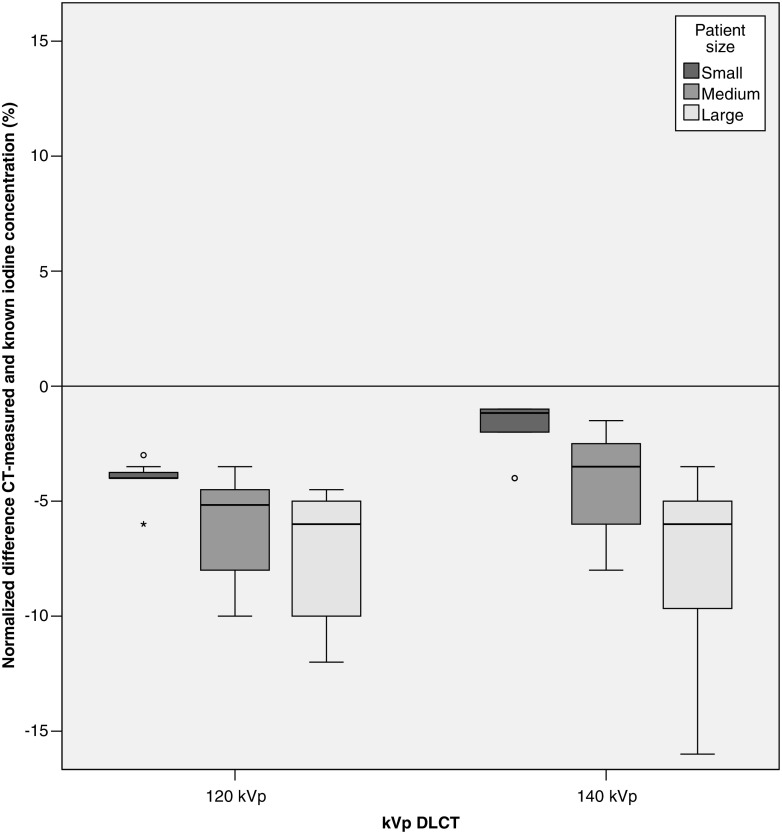
Methods: Five tubes with different iodine concentrations (0, 5, 10, 15, 20 mg/ml) were analysed in an anthropomorphic thoracic phantom. Adding two phantom rings simulated increased patient size. For third-generation dual source CT (DSCT), tube voltage combinations of 150Sn and 70, 80, 90, 100 kVp were analysed. For dual layer CT (DLCT), 120 and 140 kVp were used. Scans were repeated three times. Median normalized values and interquartile ranges (IQRs) were calculated for all kVp settings and phantom sizes.
Results: Correlation between measured and known iodine concentrations was excellent for both systems (R = 0.999-1.000, p < 0.0001). For DSCT, median measurement errors ranged from -0.5% (IQR -2.0, 2.0%) at 150Sn/70 kVp and -2.3% (IQR -4.0, -0.1%) at 150Sn/80 kVp to -4.0% (IQR -6.0, -2.8%) at 150Sn/90 kVp. For DLCT, median measurement errors ranged from -3.3% (IQR -4.9, -1.5%) at 140 kVp to -4.6% (IQR -6.0, -3.6%) at 120 kVp. Larger phantom sizes increased variability of iodine measurements (p < 0.05).
Conclusion: Iodine concentration can be accurately quantified with state-of-the-art DECT systems from two vendors. The lowest absolute errors were found for DSCT using the 150Sn/70 kVp or 150Sn/80 kVp combinations, which was slightly more accurate than 140 kVp in DLCT.
Key points: • High-end CT scanners allow accurate iodine quantification using different DECT techniques. • Lowest measurement error was found in scans with largest photon energy separation. • Dual-source CT quantified iodine slightly more accurately than dual layer CT.
Keywords: Absorptiometry, photon; Iodine; Myocardial perfusion imaging; Phantoms, imaging; Tomography, x-ray computed.
Conflict of interest statement
Guarantor
The scientific guarantor of this publication is R. Vliegenthart.
Conflict of interest
The authors B. Schmidt and T. Flohr of this manuscript declare relationships with the following company: Siemens Healthcare GmbH, Forchheim, Germany. Author J. Milles declares relationships with the following company: Philips Healthcare, Eindhoven, the Netherlands.
The other authors of this manuscript declare no relationships with any companies whose products or services may be related to the subject matter of the article.
Funding
This study has received funding by a personal grant of R. Vliegenthart from the Netherlands Organisation for Scientific Research.
Statistics and biometry
No complex statistical methods were necessary for this paper.
Ethical approval
Institutional review board approval was not required because this was a phantom study.
Methodology
• experimental
• multicentre study
Figures
References
-
- Jaarsma C, Leiner T, Bekkers SC, et al. Diagnostic performance of noninvasive myocardial perfusion imaging using single-photon emission computed tomography, cardiac magnetic resonance, and positron emission tomography imaging for the detection of obstructive coronary artery disease: a meta-analysis. J Am Coll Cardiol. 2012;59:1719–1728. doi: 10.1016/j.jacc.2011.12.040. - DOI - PubMed
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
