

Long-term follow-up after active surveillance or curative treatment: quality-of-life outcomes of men with low-risk prostate cancer
- PMID: 28168601
- PMCID: PMC5420369
- DOI: 10.1007/s11136-017-1507-7
Long-term follow-up after active surveillance or curative treatment: quality-of-life outcomes of men with low-risk prostate cancer
Abstract
Purpose: To compare long-term (4-10 years) quality of life (QoL) of men with low-risk prostate cancer (PCa) treated by different modalities and a reference group without PCa.
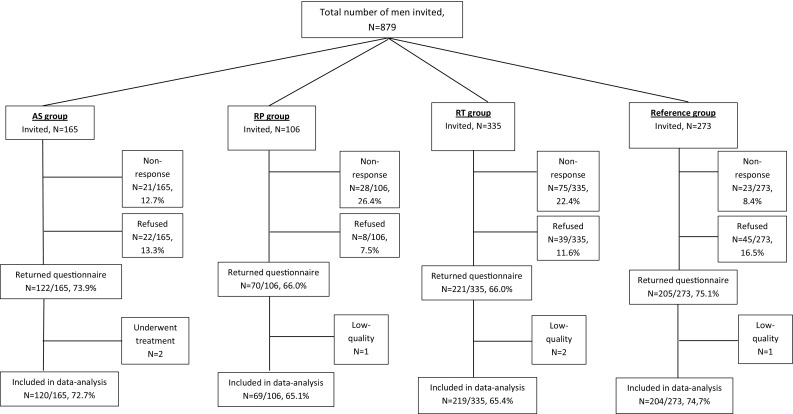
Methods: In this cross-sectional study, four groups were sent a one-time QoL-questionnaire; PCa patients (1) following the structured Prostate cancer Research International Active Surveillance protocol, (2) who underwent radical prostatectomy (RP) in the context of the European Randomized study of Screening for Prostate Cancer-section Rotterdam, (3) who underwent radiotherapy (RT) at an academic hospital in The Netherlands, and (4) an age-matched reference group of men without PCa. The QoL-questionnaire addressed prostate-specific health (EPIC), generic health (SF-12), and anxiety (STAI-6). Statistical significance (p ≤ 0.05) and clinical relevance (≥0.5 SD) of differences between groups were assessed.
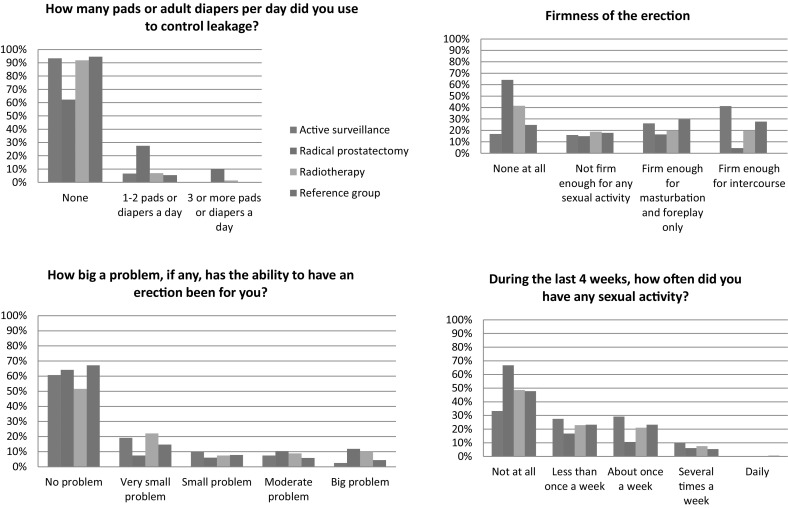
Results: The AS, RP, RT, and reference group response rates amounted to 74% (122/165), 66% (70/106), 66% (221/335), and 75% (205/273), respectively. At a mean of 6.6 years of follow-up, active surveillance (AS)-men reported better urinary function [M = 93.0 (SD = 10.6) vs. 80.0 (SD = 19.1), p ≤ 0.001], less urinary incontinence [M = 90.0 (SD = 14.6) vs. 70.1 (SD = 28.8), p ≤ 0.001], and better sexual function [M = 40.9 (SD = 24.6) vs. 14.8 (17.7), p ≤ 0.001, clinically relevant] than RP-men. Compared to RT, AS-men reported better sexual function [M = 40.9 (SD = 24.6) vs. 25.8 (SD = 25.0), p = 0.069]. The four groups reported similarly low anxiety levels; the number of highly anxious men (STAI ≥ 44) ranged from 8 to 13%. For all QoL domains, men on AS and men without PCa reported very similar scores.
Conclusions: Prostate-specific function of AS-men was significantly better than that of RP-men. When comparing AS to RT, a borderline significant difference in sexual function was seen. Men who followed an AS strategy for a long-term period were not anxious and accepted it well, suggesting that AS may be a good treatment option for men with low-risk PCa.
Keywords: Active surveillance; Patient reported outcome; Quality of life; Radical prostatectomy; Radiotherapy; Shared decision-making.
Conflict of interest statement
Conflict of interest
Venderbos declares that she has no conflict of interest. Aluwini declares that he has no conflict of interest. Roobol declares that she has no conflict of interest. Bokhorst declares that he has no conflict of interest. Oomens declares that he has no conflict of interest. Bangma declares that he has no conflict of interest. Korfage declares that she has no conflict of interest.
Sources of support
Prostate Cancer Research Foundation (SWOP), Rotterdam, The Netherlands.
Funding
This study was funded by the Prostate Cancer Research Foundation, Rotterdam, The Netherlands.
Ethical approval
All procedures performed in studies involving human participants were in accordance with the ethical standards of the institutional review board (MEC 2014-596) and with the 1964 Helsinki declaration and its later amendments or comparable ethical standards.
Informed consent
Informed consent was obtained from all individual participants included in the study.
Figures
References
-
- Sanda MG, Dunn RL, Michalski J, Sandler HM, Northouse L, Hembroff L, Lin X, Greenfield TK, Litwin MS, Saigal CS, Mahadevan A, Klein E, Kibel A, Pisters LL, Kuban D, Kaplan I, Wood D, Ciezki J, Shah N, Wei JT. Quality of life and satisfaction with outcome among prostate-cancer survivors. The New England Journal of Medicine. 2008;358(12):1250–1261. doi: 10.1056/NEJMoa074311. - DOI - PubMed
-
- Tran K, Rahal R, Fung S, Louzado C, Porter G, Xu J, Bryant H, Collaboration with the System Performance Steering, C. Technical Working, G Patterns of care and treatment trends for Canadian men with localized low-risk prostate cancer: an analysis of provincial cancer registry data. Curr Oncol. 2016;23(1):56–59. doi: 10.3747/co.23.3011. - DOI - PMC - PubMed
-
- Klotz L, Vesprini D, Sethukavalan P, Jethava V, Zhang L, Jain S, Yamamoto T, Mamedov A, Loblaw A. Long-term follow-up of a large active surveillance cohort of patients with prostate cancer. Journal of Clinical Oncology: Official Journal of the American Society of Clinical Oncology. 2015;33(3):272–277. doi: 10.1200/JCO.2014.55.1192. - DOI - PubMed
-
- Heidenreich A, Bastian PJ, Bellmunt J, Bolla M, Joniau S, van der Kwast T, Mason M, Matveev V, Wiegel T, Zattoni F, Mottet N. EAU guidelines on prostate cancer. part 1: screening, diagnosis, and local treatment with curative intent-update 2013. European urology. 2014;65(1):124–137. doi: 10.1016/j.eururo.2013.09.046. - DOI - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
