

Diffuse coronary artery disease among other atherosclerotic plaque characteristics by coronary computed tomography angiography for predicting coronary vessel-specific ischemia by fractional flow reserve
- PMID: 28168977
- PMCID: PMC5394795
- DOI: 10.1016/j.atherosclerosis.2017.01.018
Diffuse coronary artery disease among other atherosclerotic plaque characteristics by coronary computed tomography angiography for predicting coronary vessel-specific ischemia by fractional flow reserve
Abstract
Background and aims: Coronary computed tomography angiography (CCTA) permits effective identification of diffuse CAD and atherosclerotic plaque characteristics (APCs). We sought to examine the usefulness of diffuse CAD beyond luminal narrowing and APCs by CCTA to detect vessel-specific ischemia.
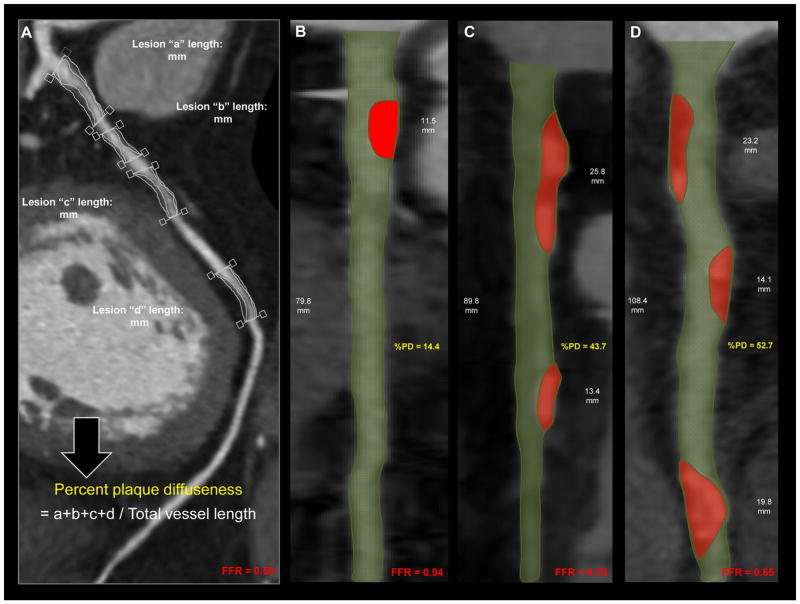
Methods: 407 vessels (n = 252 patients) from the DeFACTO diagnostic accuracy study were retrospectively analyzed for percent plaque diffuseness (PD). Percent plaque diffuseness (PD) was obtained on per-vessel level by summation of all contiguous lesion lengths and divided by total vessel length, and was logarithmically transformed (log percent PD). Additional CCTA measures of stenosis severity including minimal lumen diameter (MLD), and APCs, such as positive remodeling (PR) and low attenuation plaque (LAP), were also included. Vessel-specific ischemia was defined as fractional flow reserve (FFR) ≤0.80. Multivariable regression, discrimination by area under the receiver operating characteristic curve (AUC), and category-free net reclassification improvement (cNRI) were assessed.
Results: Backward stepwise logistic regression revealed that for every unit increase in log percent PD, there was a 58% (95% CI: 1.01-2.48, p = 0.048) rise in the odds of having an abnormal FFR, independent of stenosis severity and APCs. The AUC indicated no further improvement in discriminatory ability after adding log percent PD to the final parsimonious model of MLD, PR, and LAP (AUC difference: 0.003, 95% CI: -0.003-0.010, p = 0.33). Conversely, adding log percent PD to the base model of MLD, PR, and LAP improved cNRI by 0.21 (95% CI: 0.01-0.41, p < 0.001).
Conclusions: Accounting for diffuse CAD may help improve the accuracy of CCTA for detecting vessel-specific ischemia.
Keywords: Atherosclerotic plaque characteristics; Coronary computed tomography angiography; Diffuse coronary artery disease; Fractional flow reserve; Stenosis severity.
Copyright © 2017 The Authors. Published by Elsevier B.V. All rights reserved.
Conflict of interest statement
Dr. Min serves as a consultant to HeartFlow. All other authors have no conflicts of interest to disclose.
Figures

References
-
- Lloyd-Jones D, Adams RJ, Brown TM, et al. Executive summary: heart disease and stroke statistics--2010 update: a report from the American Heart Association. Circulation. 2010;121:948–54. - PubMed
-
- De Bruyne B, Hersbach F, Pijls NH, et al. Abnormal epicardial coronary resistance in patients with diffuse atherosclerosis but “Normal” coronary angiography. Circulation. 2001;104:2401–6. - PubMed
-
- Gould KL, Nakagawa Y, Nakagawa K, et al. Frequency and clinical implications of fluid dynamically significant diffuse coronary artery disease manifest as graded, longitudinal, base-to-apex myocardial perfusion abnormalities by noninvasive positron emission tomography. Circulation. 2000;101:1931–9. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
