

RBC Transfusion Improves Cerebral Oxygen Delivery in Subarachnoid Hemorrhage
- PMID: 28169942
- PMCID: PMC5350019
- DOI: 10.1097/CCM.0000000000002266
RBC Transfusion Improves Cerebral Oxygen Delivery in Subarachnoid Hemorrhage
Abstract
Objectives: Impaired oxygen delivery due to reduced cerebral blood flow is the hallmark of delayed cerebral ischemia following subarachnoid hemorrhage. Since anemia reduces arterial oxygen content, it further threatens oxygen delivery increasing the risk of cerebral infarction. Thus, subarachnoid hemorrhage may constitute an important exception to current restrictive transfusion practices, wherein raising hemoglobin could reduce the risk of ischemia in a critically hypoperfused organ. In this physiologic proof-of-principle study, we determined whether transfusion could augment cerebral oxygen delivery, particularly in vulnerable brain regions, across a broad range of hemoglobin values.
Design: Prospective study measuring cerebral blood flow and oxygen extraction fraction using O-PET. Vulnerable brain regions were defined as those with baseline oxygen delivery less than 4.5 mL/100 g/min.
Setting: PET facility located within the Neurology/Neurosurgery ICU.
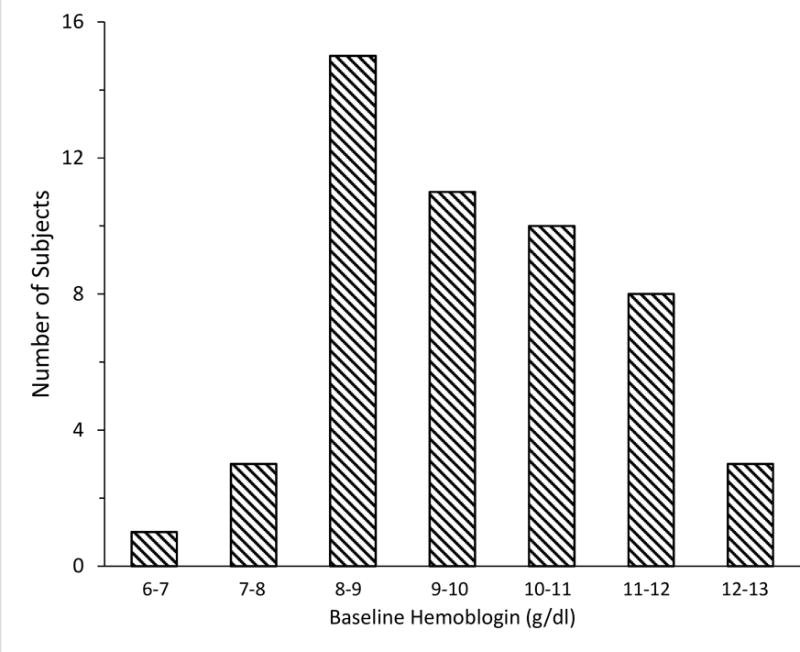
Patients: Fifty-two patients at risk for delayed cerebral ischemia after aneurysmal subarachnoid hemorrhage with hemoglobin 7-13 g/dL.
Interventions: Transfusion of one unit of RBCs over 1 hour.
Measurements and main results: Baseline hemoglobin was 9.7 g/dL (range, 6.9-12.9), and cerebral blood flow was 43 ± 11 mL/100 g/min. After transfusion, hemoglobin rose from 9.6 ± 1.4 to 10.8 ± 1.4 g/dL (12%; p < 0.001) and oxygen delivery from 5.0 (interquartile range, 4.4-6.6) to 5.5 mL/100 g/min (interquartile range, 4.8-7.0) (10%; p = 0.001); the response was comparable across the range of hemoglobin values. In vulnerable brain regions, transfusion resulted in a greater (16%) rise in oxygen delivery associated with reduction in oxygen extraction fraction, independent of Hgb level (p = 0.002 vs normal regions).
Conclusions: This study demonstrates that RBC transfusion improves cerebral oxygen delivery globally and particularly to vulnerable regions in subarachnoid hemorrhage patients at risk for delayed cerebral ischemia across a wide range of hemoglobin values and suggests that restrictive transfusion practices may not be appropriate in this population. Large prospective trials are necessary to determine if these physiologic benefits translate into clinical improvement and outweigh the risk of transfusion.
Conflict of interest statement
Figures

Comment in
-
Caution Warranted Regarding Transfusion for Subarachnoid Hemorrhage.Crit Care Med. 2017 Sep;45(9):e986-e987. doi: 10.1097/CCM.0000000000002508. Crit Care Med. 2017. PMID: 28816854 No abstract available.
-
The authors reply.Crit Care Med. 2017 Sep;45(9):e987-e988. doi: 10.1097/CCM.0000000000002532. Crit Care Med. 2017. PMID: 28816855 No abstract available.
References
-
- Grubb RL, Jr, Raichle MEME, Eichling JOO, et al. Effects of subarachnoid hemorrhage on cerebral blood volume, blood flow, and oxygen utilization in humans. Journal of Neurosurgery. 1977;46:446–453. - PubMed
-
- Levy ML, Rabb CH, Zelman V, et al. Cardiac performance enhancement from dobutamine in patients refractory to hypervolemic therapy for cerebral vasospasm. Journal of Neurosurgery. 1993;79:494–499. - PubMed
-
- Lennihan L, Mayer Sa, Fink ME, et al. Effect of hypervolemic therapy on cerebral blood flow after subarachnoid hemorrhage : a randomized controlled trial. Stroke. 2000;31:383–391. - PubMed
-
- Muench E, Horn P, Bauhuf C, et al. Effects of hypervolemia and hypertension on regional cerebral blood flow, intracranial pressure, and brain tissue oxygenation after subarachnoid hemorrhage. Critical care medicine. 2007;35:1844–1851. - PubMed
-
- Gathier CS, Dankbaar JW, van der Jagt M, et al. Effects of Induced Hypertension on Cerebral Perfusion in Delayed Cerebral Ischemia After Aneurysmal Subarachnoid Hemorrhage: A Randomized Clinical Trial. Stroke. 2015;46(11):3277–3281. - PubMed
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
