

Laparoscopic Sleeve Gastrectomy Versus Roux-Y-Gastric Bypass for Morbid Obesity-3-Year Outcomes of the Prospective Randomized Swiss Multicenter Bypass Or Sleeve Study (SM-BOSS)
- PMID: 28170356
- PMCID: PMC5300030
- DOI: 10.1097/SLA.0000000000001929
Laparoscopic Sleeve Gastrectomy Versus Roux-Y-Gastric Bypass for Morbid Obesity-3-Year Outcomes of the Prospective Randomized Swiss Multicenter Bypass Or Sleeve Study (SM-BOSS)
Abstract
Objective: Laparoscopic sleeve gastrectomy (LSG) is performed almost as often in Europe as laparoscopic Roux-Y-Gastric Bypass (LRYGB). We present the 3-year interim results of the 5-year prospective, randomized trial comparing the 2 procedures (Swiss Multicentre Bypass Or Sleeve Study; SM-BOSS).
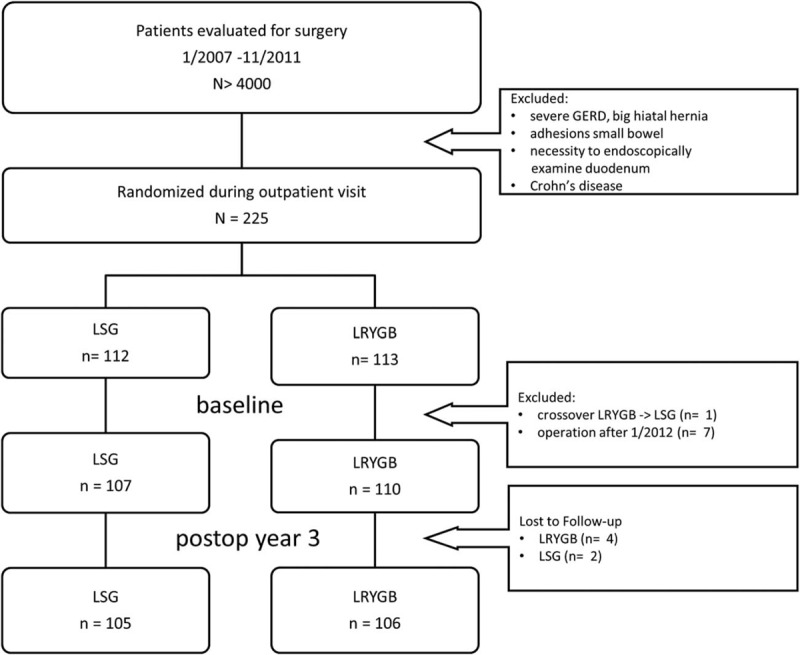
Methods: Initially, 217 patients (LSG, n = 107; LRYGB, n = 110) were randomized to receive either LSG or LRYGB at 4 bariatric centers in Switzerland. Mean body mass index of all patients was 44 ± 11 kg/m, mean age was 43 ± 5.3 years, and 72% of patients were female. Minimal follow-up was 3 years with a rate of 97%. Both groups were compared for weight loss, comorbidities, quality of life, and complications.
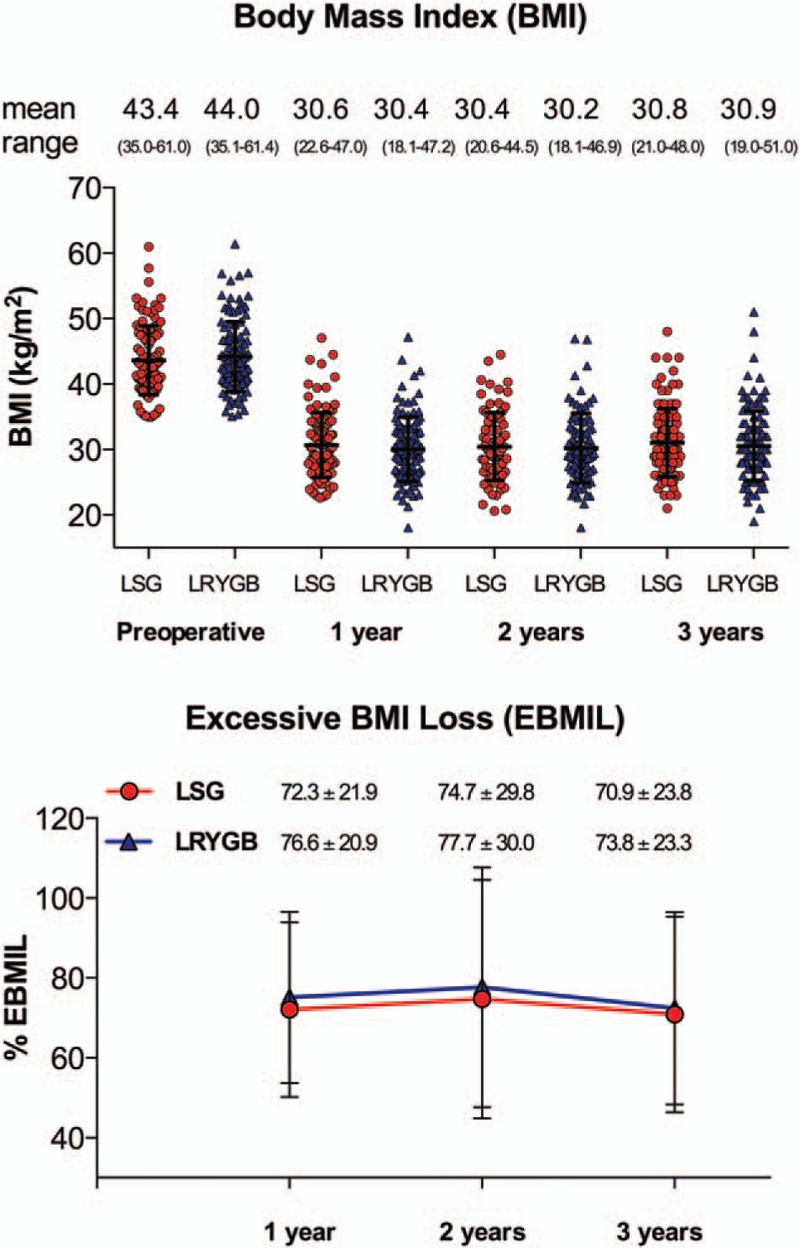
Results: Excessive body mass index loss was similar between LSG and LRYGB at each time point (1 year: 72.3 ± 21.9% vs. 76.6 ± 20.9%, P = 0.139; 2 years: 74.7 ± 29.8% vs. 77.7 ± 30%, P = 0.513; 3 years: 70.9 ± 23.8% vs. 73.8 ± 23.3%, P = 0.316). At this interim 3-year time point, comorbidities were significantly reduced and comparable after both procedures except for gastro-esophageal reflux disease and dyslipidemia, which were more successfully treated by LRYGB. Quality of life increased significantly in both groups after 1, 2, and 3 years postsurgery. There was no statistically significant difference in number of complications treated by reoperation (LSG, n = 9; LRYGB, n = 16, P = 0.15) or number of complications treated conservatively.
Conclusions: In this trial, LSG and LRYGB are equally efficient regarding weight loss, quality of life, and complications up to 3 years postsurgery. Improvement of comorbidities is similar except for gastro-esophageal reflux disease and dyslipidemia that appear to be more successfully treated by LRYGB.
Conflict of interest statement
The authors report no conflicts of interest.
Figures
Comment in
-
Are Guidelines for Standardized Outcome Reporting in Bariatric Surgery Responsible for Missing the Big Picture in Bariatric Surgery Related Major Complications?Ann Surg. 2018 Jul;268(1):e12-e13. doi: 10.1097/SLA.0000000000002314. Ann Surg. 2018. PMID: 28549008 No abstract available.
-
Response to: "Are Guidelines for Standardized Outcome Reporting in Bariatric Surgery Responsible for Missing the Big Picture in Bariatric Surgery Related Major Complications?".Ann Surg. 2018 Jul;268(1):e13-e14. doi: 10.1097/SLA.0000000000002317. Ann Surg. 2018. PMID: 29889680 No abstract available.
References
-
- Sjostrom L. Review of the key results from the Swedish Obese Subjects (SOS) trial—a prospective controlled intervention study of bariatric surgery. J Intern Med 2013; 273:219–234. - PubMed
-
- Angrisani L, Santonicola A, Iovino P, et al. Bariatric surgery worldwide 2013. Obes Surg 2015; 25:1822–1832. - PubMed
-
- Wolnerhanssen BK, Peters T, Kern B, et al. Predictors of outcome in treatment of morbid obesity by laparoscopic adjustable gastric banding: results of a prospective study of 380 patients. Surg Obes Relat Dis 2008; 4:500–506. - PubMed
-
- Peterli R, Wolnerhanssen BK, Peters T, et al. Prospective study of a two-stage operative concept in the treatment of morbid obesity: primary lap-band followed if needed by sleeve gastrectomy with duodenal switch. Obes Surg 2007; 17:334–340. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
