

Longitudinal assessment of sputum microbiome by sequencing of the 16S rRNA gene in non-cystic fibrosis bronchiectasis patients
- PMID: 28170403
- PMCID: PMC5295668
- DOI: 10.1371/journal.pone.0170622
Longitudinal assessment of sputum microbiome by sequencing of the 16S rRNA gene in non-cystic fibrosis bronchiectasis patients
Abstract
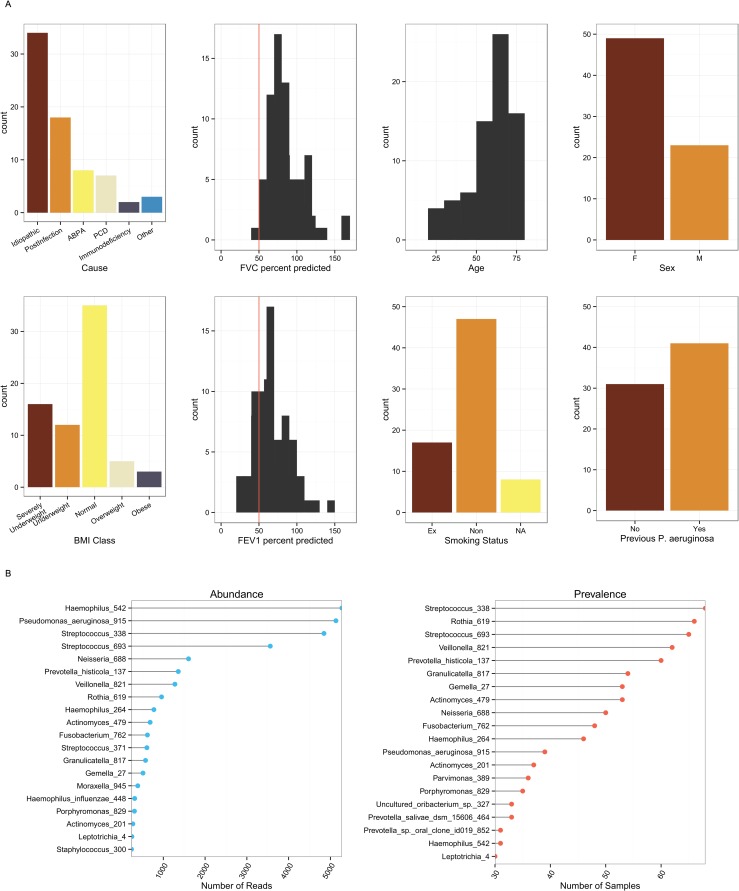
Background: Bronchiectasis is accompanied by chronic bronchial infection that may drive disease progression. However, the evidence base for antibiotic therapy is limited. DNA based methods offer better identification and quantification of microbial constituents of sputum than standard clinical culture and may help inform patient management strategies. Our study objective was to determine the longitudinal variability of the non-cystic fibrosis (CF) bronchiectasis microbiome in sputum with respect to clinical variables. Eighty-five patients with non-CF bronchiectasis and daily sputum production were recruited from outpatient clinics and followed for six months. Monthly sputum samples and clinical measurements were taken, together with additional samples during exacerbations. 16S rRNA gene sequencing of the sputum microbiota was successful for 381 samples from 76 patients and analysed in conjunction with clinical data.
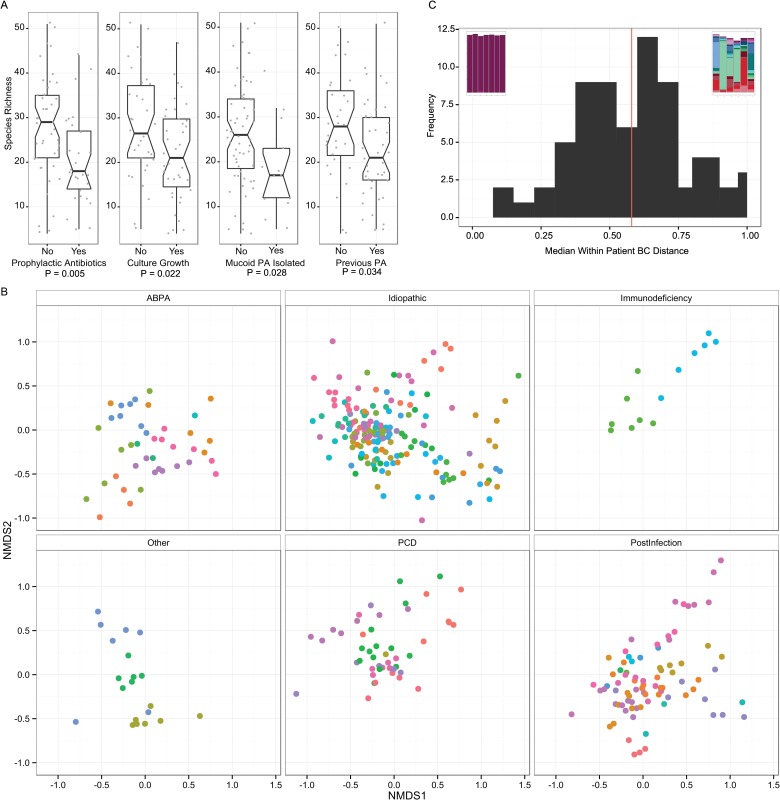
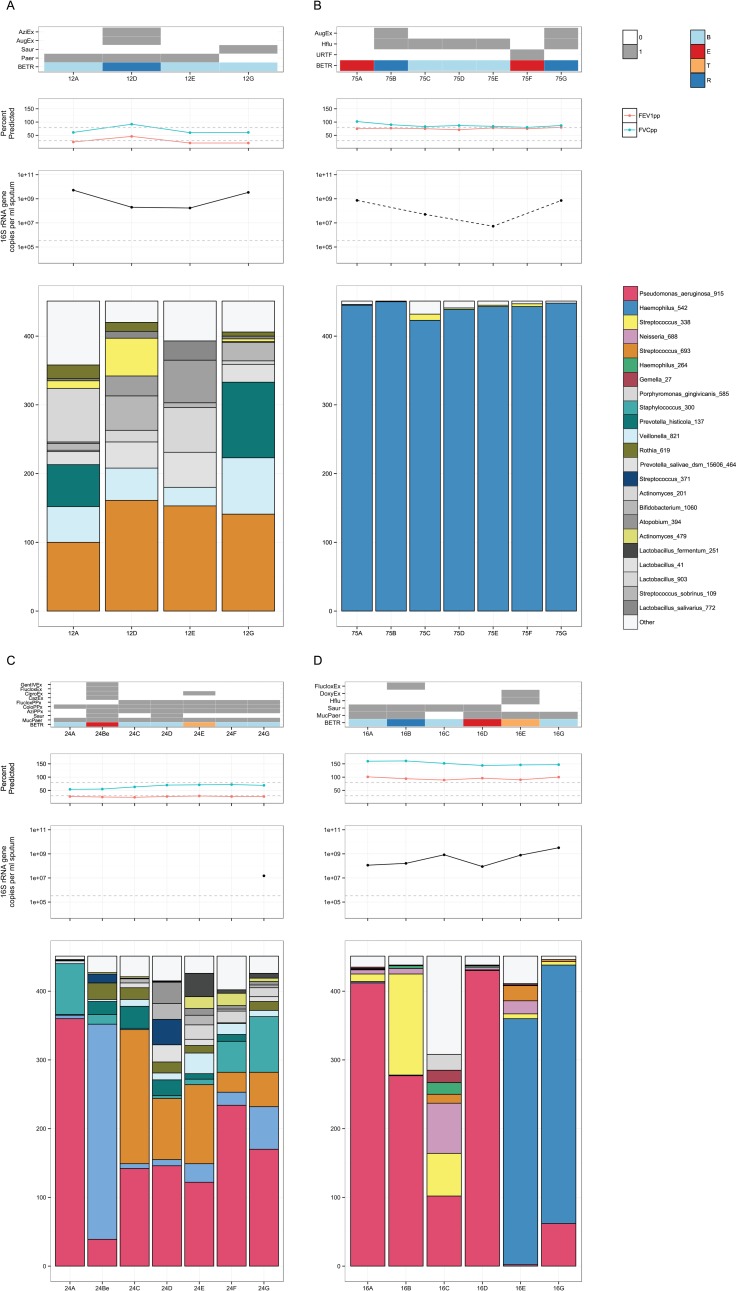
Results: Microbial communities were highly individual in composition and stability, usually with limited diversity and often containing multiple pathogens. When compared to DNA sequencing, microbial culture had restricted sensitivity in identifying common pathogens such as Pseudomonas aeruginosa, Haemophilus influenzae, Moraxella catarrhalis. With some exceptions, community characteristics showed poor correlations with clinical features including underlying disease, antibiotic use and exacerbations, with the subject showing the strongest association with community structure. When present, the pathogens mucoid Pseudomonas aeruginosa and Haemophilus influenzae may also shape the structure of the rest of the microbial community.
Conclusions: The use of microbial community analysis of sputum added to information from microbial culture. A simple model of exacerbations driven by bacterial overgrowth was not supported, suggesting a need for revision of principles for antibiotic therapy. In individual patients, the management of chronic bronchial infection may be improved by therapy specific to their microbiome, taking into account pathogen load, community stability, and acute and chronic community responses to antibiotics.
Conflict of interest statement
DB received a grant from Novartis UK for sequencing costs. The funder had no involvement in study design, collection or analysis of data, or in the decision to publish. This does not alter our adherence to PLOS ONE policies on sharing data and materials.
Figures
References
-
- Pasteur MC, Bilton D, Hill AT, on behalf of the British Thoracic Society Bronchiectasis (non-CF) Guideline Group. British Thoracic Society guideline for non-CFbronchiectasis. Thorax. 2010. July 13;65(Suppl 1):i1–i58. - PubMed
-
- Tunney MM, Klem ER, Fodor AA, Gilpin DF, Moriarty TF, McGrath SJ, et al. Use of culture and molecular analysis to determine the effect of antibiotic treatment on microbial community diversity and abundance during exacerbation in patients with cystic fibrosis. Thorax. 2011. June 15;66(7):579–84. 10.1136/thx.2010.137281 - DOI - PMC - PubMed
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
