

Vernakalant is superior to ibutilide for achieving sinus rhythm in patients with recent-onset atrial fibrillation: a randomized controlled trial at the emergency department
- PMID: 28175295
- PMCID: PMC5400093
- DOI: 10.1093/europace/euw052
Vernakalant is superior to ibutilide for achieving sinus rhythm in patients with recent-onset atrial fibrillation: a randomized controlled trial at the emergency department
Abstract
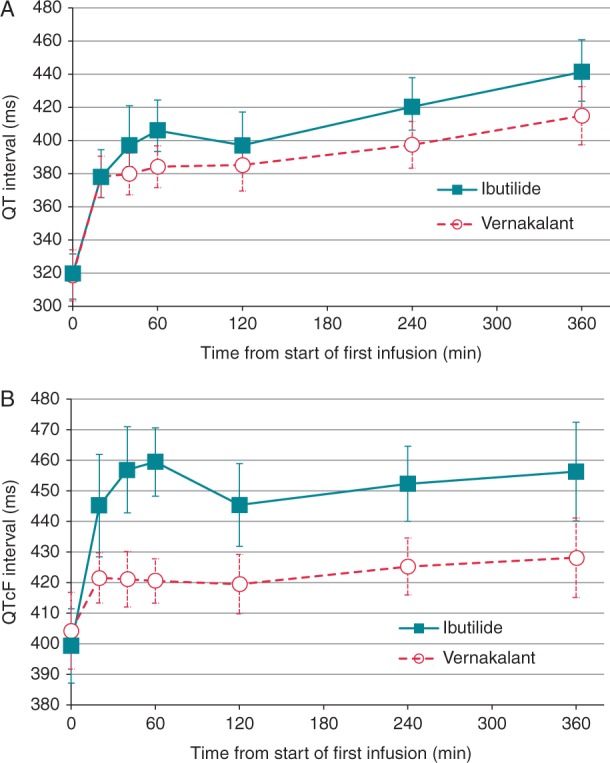
Aims: Ibutilide is a rapid-acting antiarrhythmic drug with worldwide use for conversion of recent-onset atrial fibrillation. Vernakalant, approved in the EU in 2010, is likewise used intravenously, with proven efficacy and safety compared with placebo and amiodarone in randomized clinical trials. The aim of our study was to compare the time to conversion and the conversion rate within 90 min in patients with recent-onset atrial fibrillation treated with vernakalant or ibutilide.
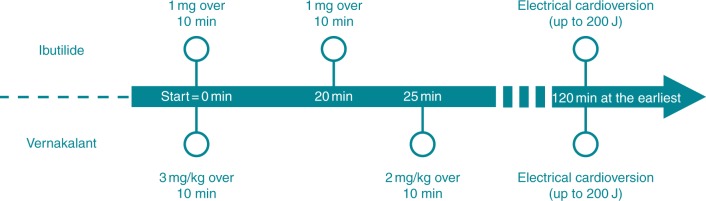
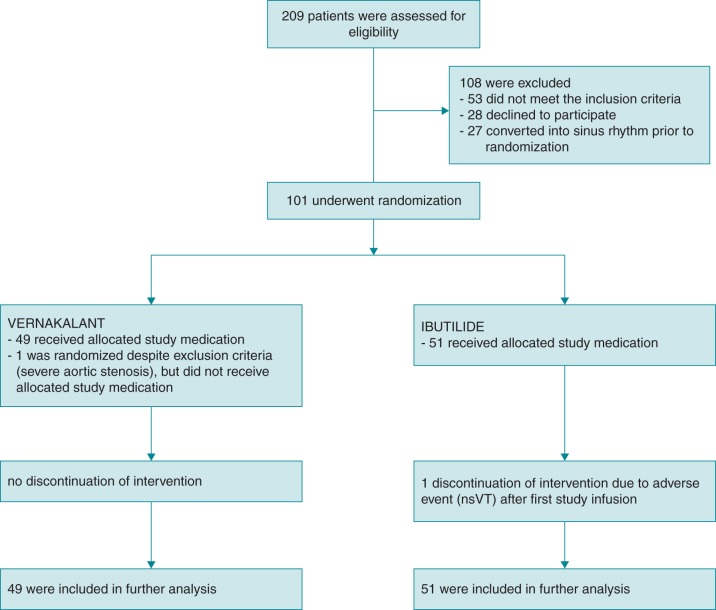
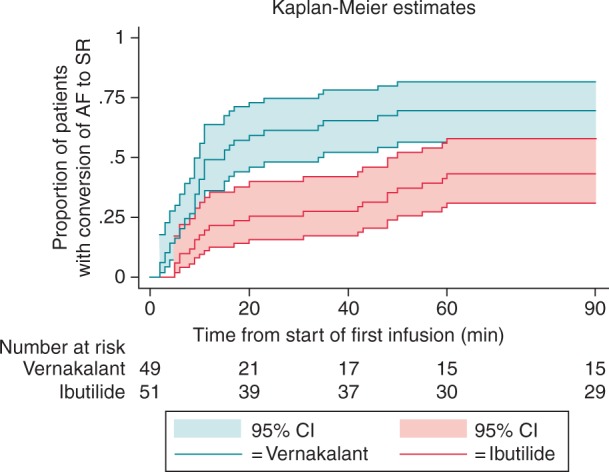
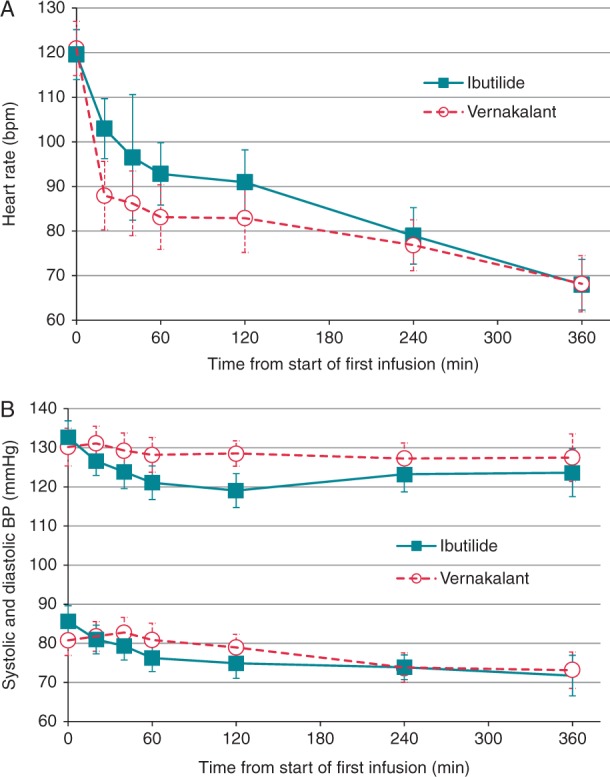
Methods and results: A randomized controlled trial registered at clinicaltrials.gov (NCT01447862) was performed in 100 patients with recent-onset atrial fibrillation treated at the emergency department of a tertiary care hospital. Patients received up to two short infusions of vernakalant (n = 49; 3 mg/kg followed by 2 mg/kg if necessary) or ibutilide (n = 51; 1 mg followed by another 1 mg if necessary) according to the manufacturer's instructions. Clinical and laboratory variables, adverse events, conversion rates, and time to conversion were recorded. Time to conversion of AF to sinus rhythm was significantly shorter in the vernakalant group compared with the ibutilide group (median time: 10 vs. 26 min, P = 0.01), and likewise the conversion success within 90 min was significantly higher in the vernakalant group (69 vs. 43%, log-rank P = 0.002). No serious adverse events occurred.
Conclusion: Vernakalant was superior to ibutilide in converting recent-onset atrial fibrillation to sinus rhythm in the emergency department setting.
Figures
Similar articles
-
Chemical cardioversion of recent-onset atrial fibrillation in the emergency department using vernakalant hydrochloride achieves safe and rapid restoration of sinus rhythm and facilitates same day discharge.Ir J Med Sci. 2017 Nov;186(4):903-908. doi: 10.1007/s11845-017-1576-1. Epub 2017 Feb 6. Ir J Med Sci. 2017. PMID: 28168639
-
Flecainide versus vernakalant for conversion of recent-onset atrial fibrillation.Int J Cardiol. 2013 Oct 3;168(3):2423-5. doi: 10.1016/j.ijcard.2013.02.006. Epub 2013 Mar 19. Int J Cardiol. 2013. PMID: 23518212
-
Propafenone versus vernakalant for conversion of recent-onset atrial fibrillation.Cardiovasc Ther. 2013 Dec;31(6):377-80. doi: 10.1111/1755-5922.12036. Cardiovasc Ther. 2013. PMID: 23683253 Clinical Trial.
-
Intravenous vernakalant: a review of its use in the management of recent-onset atrial fibrillation.Drugs. 2011 Jan 22;71(2):237-52. doi: 10.2165/10489050-000000000-00000. Drugs. 2011. PMID: 21275448 Review.
-
Pharmacological cardioversion of atrial fibrillation with vernakalant: evidence in support of the ESC Guidelines.Europace. 2014 Feb;16(2):162-73. doi: 10.1093/europace/eut274. Epub 2013 Oct 9. Europace. 2014. PMID: 24108230 Review.
Cited by
-
Pharmacologic Cardioversion in Patients with Paroxysmal Atrial Fibrillation: A Network Meta-Analysis.Cardiovasc Drugs Ther. 2021 Apr;35(2):293-308. doi: 10.1007/s10557-020-07127-1. Epub 2021 Jan 5. Cardiovasc Drugs Ther. 2021. PMID: 33400054
-
Revisiting Antiarrhythmic Drug Therapy for Atrial Fibrillation: Reviewing Lessons Learned and Redefining Therapeutic Paradigms.Front Pharmacol. 2020 Nov 9;11:581837. doi: 10.3389/fphar.2020.581837. eCollection 2020. Front Pharmacol. 2020. PMID: 33240090 Free PMC article. Review.
-
Current Drug Treatment Strategies for Atrial Fibrillation and TASK-1 Inhibition as an Emerging Novel Therapy Option.Front Pharmacol. 2021 Mar 4;12:638445. doi: 10.3389/fphar.2021.638445. eCollection 2021. Front Pharmacol. 2021. PMID: 33897427 Free PMC article. Review.
-
Clinical decision support to Optimize Care of patients with Atrial Fibrillation or flutter in the Emergency department: protocol of a stepped-wedge cluster randomized pragmatic trial (O'CAFÉ trial).Trials. 2023 Mar 31;24(1):246. doi: 10.1186/s13063-023-07230-2. Trials. 2023. PMID: 37004068 Free PMC article.
-
Efficacy and safety of intravenous vernakalant for the rapid conversion of recent-onset atrial fibrillation: A meta-analysis.Ann Noninvasive Electrocardiol. 2018 May;23(3):e12508. doi: 10.1111/anec.12508. Epub 2017 Nov 4. Ann Noninvasive Electrocardiol. 2018. PMID: 29105209 Free PMC article.
References
-
- Pedersen OD, Søndergaard P, Nielsen T, Nielsen SJ, Nielsen ES, Falstie-Jensen N et al. , DIAMOND Study Group Investigators. Atrial fibrillation, ischaemic heart disease, and the risk of death in patients with heart failure. Eur Heart J 2006;27:2866–70. - PubMed
-
- McNamara RL, Tamariz LJ, Segal JB, Bass EB. Management of atrial fibrillation: review of the evidence for the role of pharmacologic therapy, electrical cardioversion, and echocardiography. Ann Intern Med 2003;139:1018–33. - PubMed
-
- Foster RH, Wilde MI, Markham A. Ibutilide: a review of its pharmacological properties and clinical potential in the acute management of atrial flutter and fibrillation. Drugs 1997;54:312–30. - PubMed
Publication types
MeSH terms
Substances
Associated data
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
