

Middle East Respiratory Syndrome
- PMID: 28177862
- PMCID: PMC5362064
- DOI: 10.1056/NEJMsr1408795
Middle East Respiratory Syndrome
Abstract
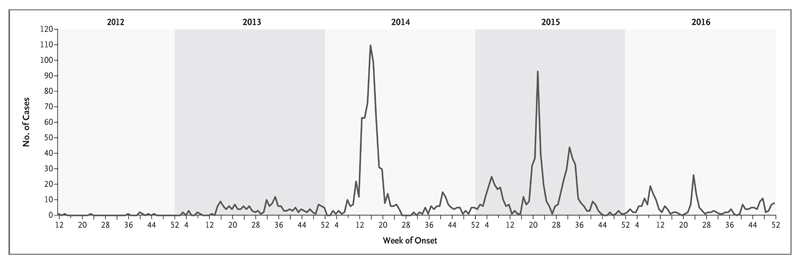
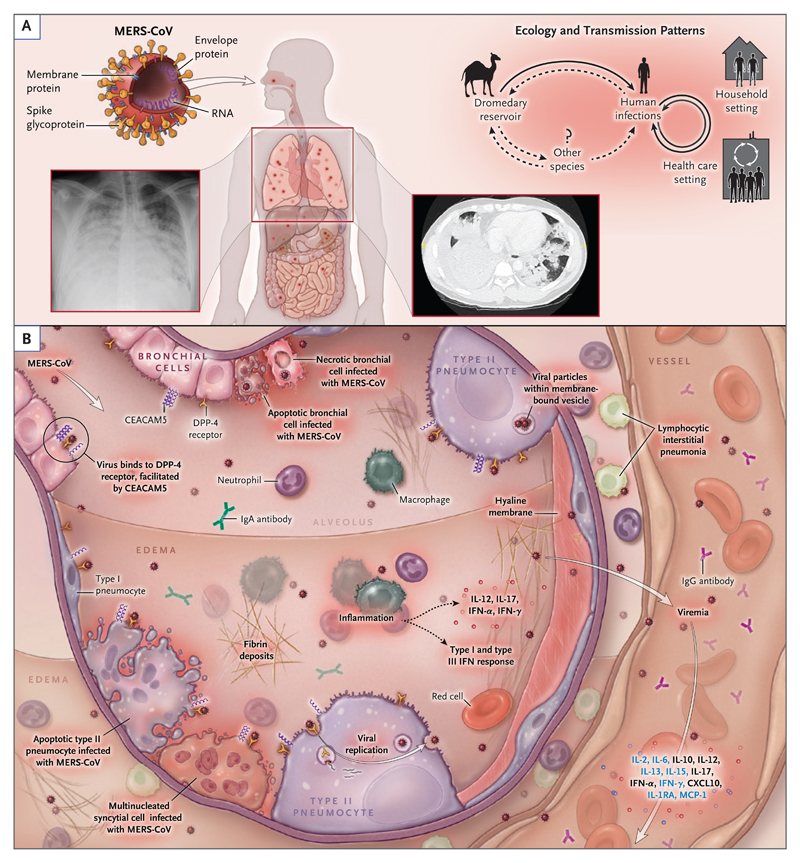
Between September 2012 and January 20, 2017, the World Health Organization (WHO) received reports from 27 countries of 1879 laboratory-confirmed cases in humans of the Middle East respiratory syndrome (MERS) caused by infection with the MERS coronavirus (MERS-CoV) and at least 659 related deaths. Cases of MERS-CoV infection continue to occur, including sporadic zoonotic infections in humans across the Arabian Peninsula, occasional importations and associated clusters in other regions, and outbreaks of nonsustained human-to-human transmission in health care settings. Dromedary camels are considered to be the most likely source of animal-to-human transmission. MERS-CoV enters host cells after binding the dipeptidyl peptidase 4 (DPP-4) receptor and the carcinoembryonic antigen–related cell-adhesion molecule 5 (CEACAM5) cofactor ligand, and it replicates efficiently in the human respiratory epithelium. Illness begins after an incubation period of 2 to 14 days and frequently results in hypoxemic respiratory failure and the need for multiorgan support. However, asymptomatic and mild cases also occur. Real-time reverse-transcription–polymerase-chain-reaction (RT-PCR) testing of respiratory secretions is the mainstay for diagnosis, and samples from the lower respiratory tract have the greatest yield among seriously ill patients. There is no antiviral therapy of proven efficacy, and thus treatment remains largely supportive; potential vaccines are at an early developmental stage. There are multiple gaps in knowledge regarding the evolution and transmission of the virus, disease pathogenesis, treatment, and prospects for a vaccine. The ongoing occurrence of MERS in humans and the associated high mortality call for a continued collaborative approach toward gaining a better understanding of the infection both in humans and in animals.
MERS-CoV was first identified in September 2012 in a patient from Saudi Arabia who had hypoxemic respiratory failure and multiorgan illness. Subsequent cases have included infections in humans across the Arabian Peninsula, occasional importations and associated clusters in other regions, and outbreaks of nonsustained human-to-human transmission in health care settings (Fig. 1).
Figures

References
-
- Zaki AM, van Boheemen S, Bestebroer TM, Osterhaus ADME, Fouchier RAM. Isolation of a novel coronavirus from a man with pneumonia in Saudi Arabia. N Engl J Med. 2012;367:1814–20. - PubMed
-
- World Health Organization. Middle East respiratory syndrome coronavirus (MERS-CoV) ( http://www.who.int/emergencies/mers-cov/en/)
-
- Azhar EI, El-Kafrawy SA, Farraj SA, et al. Evidence for camel-to-human transmission of MERS coronavirus. N Engl J Med. 2014;370:2499–505. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous