

Use of susceptibility-weighted imaging in assessing ischemic penumbra: A case report
- PMID: 28178170
- PMCID: PMC5313027
- DOI: 10.1097/MD.0000000000006091
Use of susceptibility-weighted imaging in assessing ischemic penumbra: A case report
Abstract
Rationale: The ischemic penumbra assessment is essential for the subsequent therapy and prediction of evolution in patients with acute ischemic infraction. Although controversial as a perfect equivalence to penumbra, perfusion-weighted imaging (PWI)-diffusion-weighted imaging (DWI) mismatch may predict the response to thrombolysis. Due to the reliance of PWI on contrast agents, noninvasive alternatives remain an unmet need.
Patient concerns: We reported a 65-year-old man complained of paroxysmal hemiplegia of his right limbs and anepia for 2 days, whereas the symptoms lasted for about 12 hours when he admitted to the hospital.
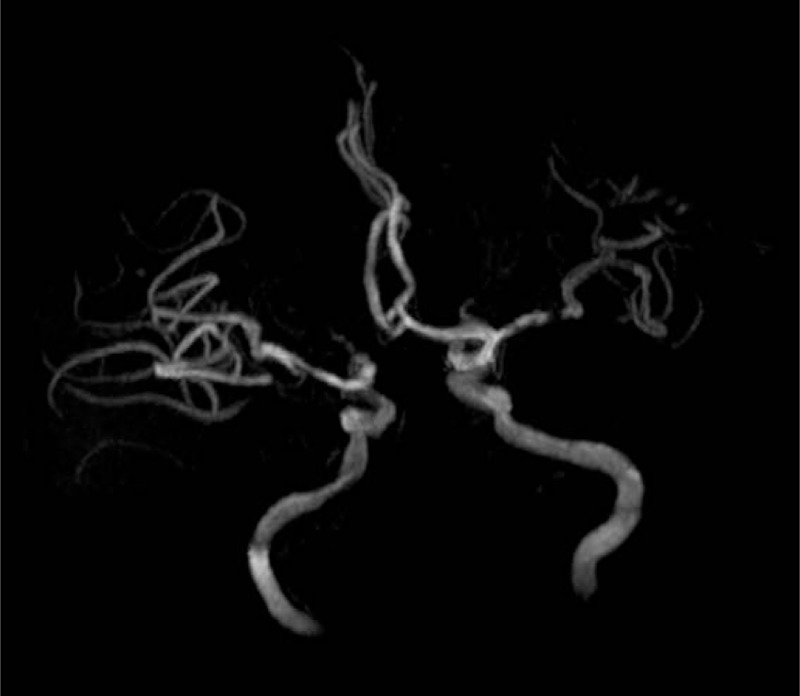
Diagnosis: We diagnosed it as acute ischemic stroke caused by the left middle cerebral artery stenosis.
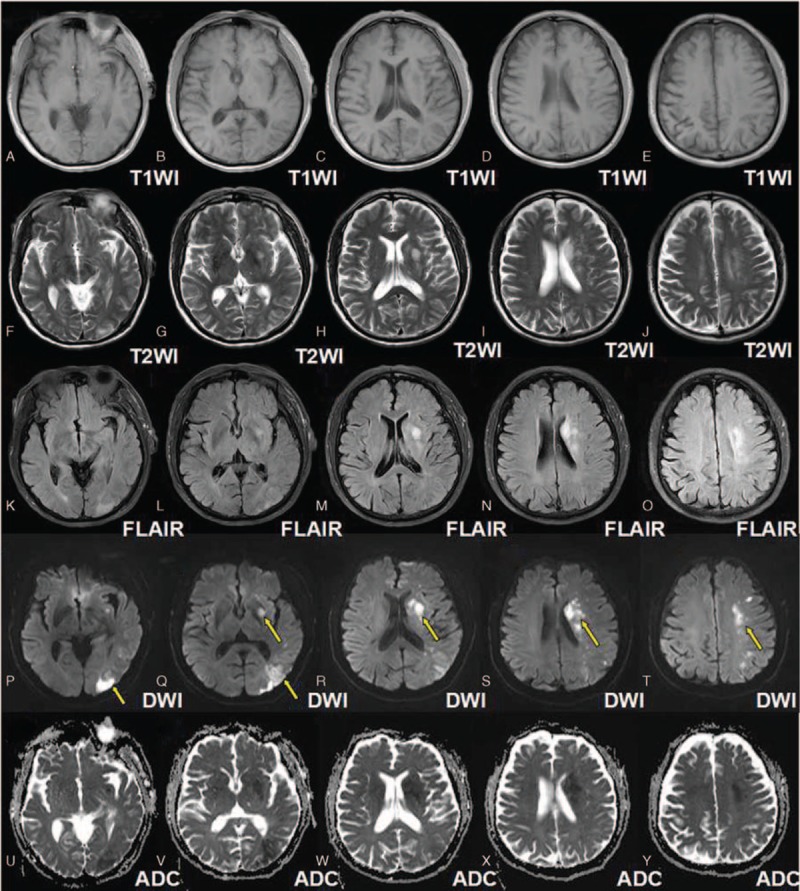
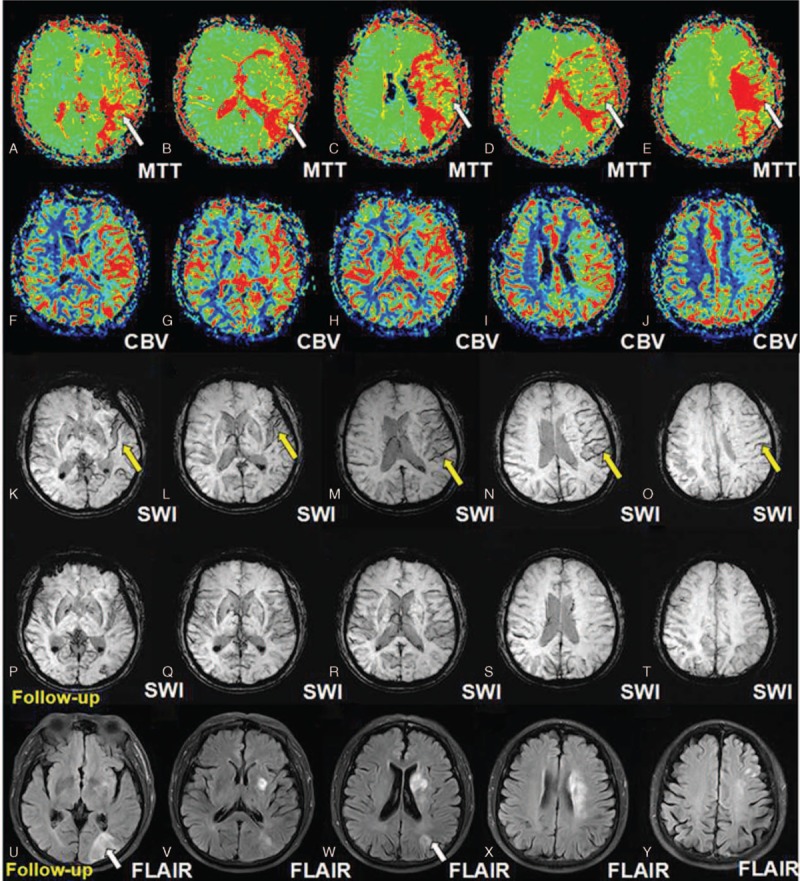
Interventions: Susceptibility-weighted imaging (SWI), multimodal magnetic resonance imaging (MRI) work-up which includes conventional MRI sequences (T1WI, T2WI, and FLAIR), DWI, PWI.
Outcomes: His DWI-SWI mismatch was comparable to that of DWI-PWI at admission, suggesting that DWI-SWI could predict ischemic penumbra in patient with acute infarction. He refused the digital subtraction angiography examination or stenting, and he was treated with aspirin, atorvastain, and supportive treatment. The patient received a reexamination of the conventional MRI and SWI 11 days later. Expansion of the infarction in the affected MCA territory resulted from the penumbra indicated by the mismatch between DWI-SWI.
Lessons: SWI can be used as a noninvasive alternative to evaluate the ischemic penumbra. Besides, SWI can provide perfusion information comparable to PWI and SWI is sufficient to identify occlusive arteries.
Conflict of interest statement
The authors have no conflicts of interest to disclose.
Figures
References
-
- Hermier M, Nighoghossian N. Contribution of susceptibility-weighted imaging to acute stroke assessment. Stroke 2004;35:1989–94. - PubMed
-
- Sun W, Liu W, Zhang Z, et al. Asymmetrical cortical vessel sign on susceptibility-weighted imaging: a novel imaging marker for early neurological deterioration and unfavorable prognosis. Eur J Neurol 2014;21:1411–8. - PubMed
-
- Meoded A, Poretti A, Benson JE, et al. Evaluation of the ischemic penumbra focusing on the venous drainage: the role of susceptibility weighted imaging (SWI) in pediatric ischemic cerebral stroke. J Neuroradiol 2014;41:108–16. - PubMed
-
- Kesavadas C, Santhosh K, Thomas B. Susceptibility weighted imaging in cerebral hypoperfusion-can we predict increased oxygen extraction fraction? Neuroradiology 2010;5:1047–54. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
