

Benefits of ultra-fast-track anesthesia in left ventricular assist device implantation: a retrospective, propensity score matched cohort study of a four-year single center experience
- PMID: 28179009
- PMCID: PMC5299681
- DOI: 10.1186/s13019-017-0573-9
Benefits of ultra-fast-track anesthesia in left ventricular assist device implantation: a retrospective, propensity score matched cohort study of a four-year single center experience
Abstract
Background: The use of left ventricular assist devices (LVADs) has gained significant importance for treatment of end-stage heart failure. Fast-track procedures are well established in cardiac surgery, whereas knowledge of their benefits after LVAD implantation is sparse. We hypothesized that ultra-fast-track anesthesia (UFTA) with in-theater extubation or at a maximum of 4 h. after surgery is feasible in Interagency Registry for Mechanically Assisted Circulatory Support (INTERMACS) level 3 and 4 patients and might prevent postoperative complications.
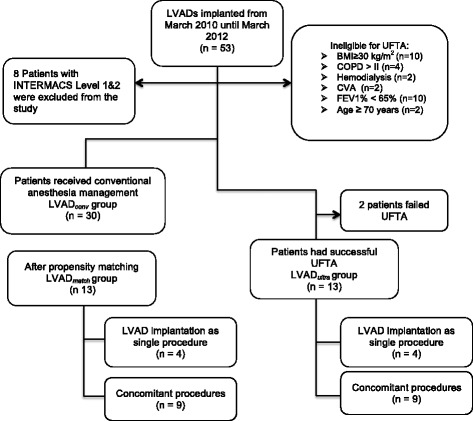
Methods: From March, 2010 to March, 2012, 53 LVADs (50 Heart Mate II and 3 Heart Ware) were implanted in patients in our department. UFTA was successfully performed (LVAD ultra ) in 13 patients. After propensity score matching, we compared the LVAD ultra group with a matched group (LVAD match ) receiving conventional anesthesia management.
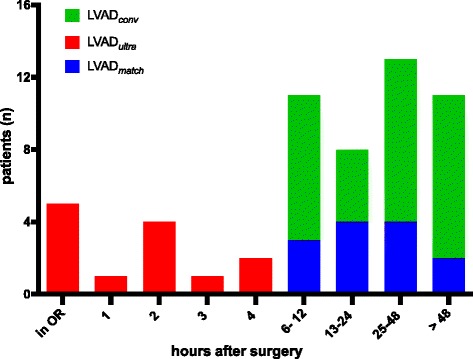
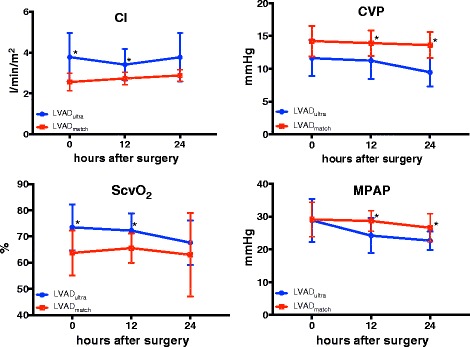
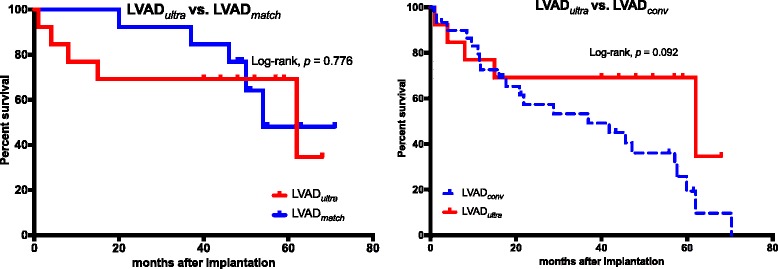
Results: Patients in the LVAD ultra group had significantly lower incidences of pneumonia (p = 0.031), delirium (p = 0.031) and right ventricular failure (RVF) (p = 0.031). They showed a significantly higher cardiac index in the first 12 h. (p = 0.017); a significantly lower central venous pressure during the first 24 h. postoperatively (p = 0.005) and a significantly shorter intensive care unit (ICU) stay (p = 0.016). Kaplan-Meier analysis after four years of follow-up showed no significant difference in survival.
Conclusion: In this pilot study, we demonstrated the feasibility of ultra-fast-track anesthesia in LVAD implantation in selected patients with INTERMACS level 3-4. Patients had a lower incidence of postoperative complications, better hemodynamic performance, shorter length of ICU stay and lower incidence of RVF after UFTA. Prospective randomized investigations should examine the preservation of right ventricular function in larger numbers and identify appropriate selection criteria.
Keywords: Fast-track-anesthesia; Left ventricular assist device; Postoperative complication; Right ventricular failure.
Figures
Similar articles
-
Early Right Ventricular Assist Device Use in Patients Undergoing Continuous-Flow Left Ventricular Assist Device Implantation: Incidence and Risk Factors From the Interagency Registry for Mechanically Assisted Circulatory Support.Circ Heart Fail. 2017 Oct;10(10):e003863. doi: 10.1161/CIRCHEARTFAILURE.117.003863. Circ Heart Fail. 2017. PMID: 29021348 Free PMC article.
-
Less invasive left ventricular assist device implantation may reduce right ventricular failure.Interact Cardiovasc Thorac Surg. 2019 Oct 1;29(4):592-598. doi: 10.1093/icvts/ivz143. Interact Cardiovasc Thorac Surg. 2019. PMID: 31326991
-
Novel percutaneous dual-lumen cannula-based right ventricular assist device provides effective support for refractory right ventricular failure after left ventricular assist device implantation.Interact Cardiovasc Thorac Surg. 2020 Apr 1;30(4):499-506. doi: 10.1093/icvts/ivz322. Interact Cardiovasc Thorac Surg. 2020. PMID: 31986207
-
Left ventricular vs. biventricular mechanical support: Decision making and strategies for avoidance of right heart failure after left ventricular assist device implantation.Int J Cardiol. 2015 Nov 1;198:241-50. doi: 10.1016/j.ijcard.2015.06.103. Epub 2015 Jul 2. Int J Cardiol. 2015. PMID: 26232775 Review.
-
Predicting the Risk of Right Ventricular Failure in Patients Undergoing Left Ventricular Assist Device Implantation: A Systematic Review.Circ Heart Fail. 2020 Oct;13(10):e006994. doi: 10.1161/CIRCHEARTFAILURE.120.006994. Epub 2020 Sep 28. Circ Heart Fail. 2020. PMID: 32981331
Cited by
-
Center Variation in Medicare Spending for Durable Left Ventricular Assist Device Implant Hospitalizations.JAMA Cardiol. 2019 Feb 1;4(2):153-160. doi: 10.1001/jamacardio.2018.4717. JAMA Cardiol. 2019. PMID: 30698605 Free PMC article.
-
[Mechanical circulatory support in terminal heart failure].Anaesthesist. 2018 May;67(5):326-335. doi: 10.1007/s00101-018-0435-4. Anaesthesist. 2018. PMID: 29623383 Review. German.
-
Prediction, prevention, and management of right ventricular failure after left ventricular assist device implantation: A comprehensive review.Front Cardiovasc Med. 2022 Nov 3;9:1040251. doi: 10.3389/fcvm.2022.1040251. eCollection 2022. Front Cardiovasc Med. 2022. PMID: 36407460 Free PMC article. Review.
-
Benefits of ultra-fast-track anesthesia for children with congenital heart disease undergoing cardiac surgery.BMC Pediatr. 2019 Dec 11;19(1):487. doi: 10.1186/s12887-019-1832-9. BMC Pediatr. 2019. PMID: 31829170 Free PMC article. Clinical Trial.
-
Clinical effect of dexmedetomidine combined with sufentanil on postoperative analgesia for transthoracic device closure of ventricular septal defects in children with ultrafast track anesthesia.J Cardiothorac Surg. 2021 Jul 28;16(1):206. doi: 10.1186/s13019-021-01592-x. J Cardiothorac Surg. 2021. PMID: 34321062 Free PMC article.
References
-
- Zhu F, Lee A, Chee YE. Fast-track cardiac care for adult cardiac surgical patients. Cochrane Database Syst Rev. 2012;10:CD003587. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
