

Prenatal stress-immune programming of sex differences in comorbidity of depression and obesity/metabolic syndrome
- PMID: 28179814
- PMCID: PMC5286728
- DOI: 10.31887/DCNS.2016.18.4/jgoldstein
Prenatal stress-immune programming of sex differences in comorbidity of depression and obesity/metabolic syndrome
Abstract
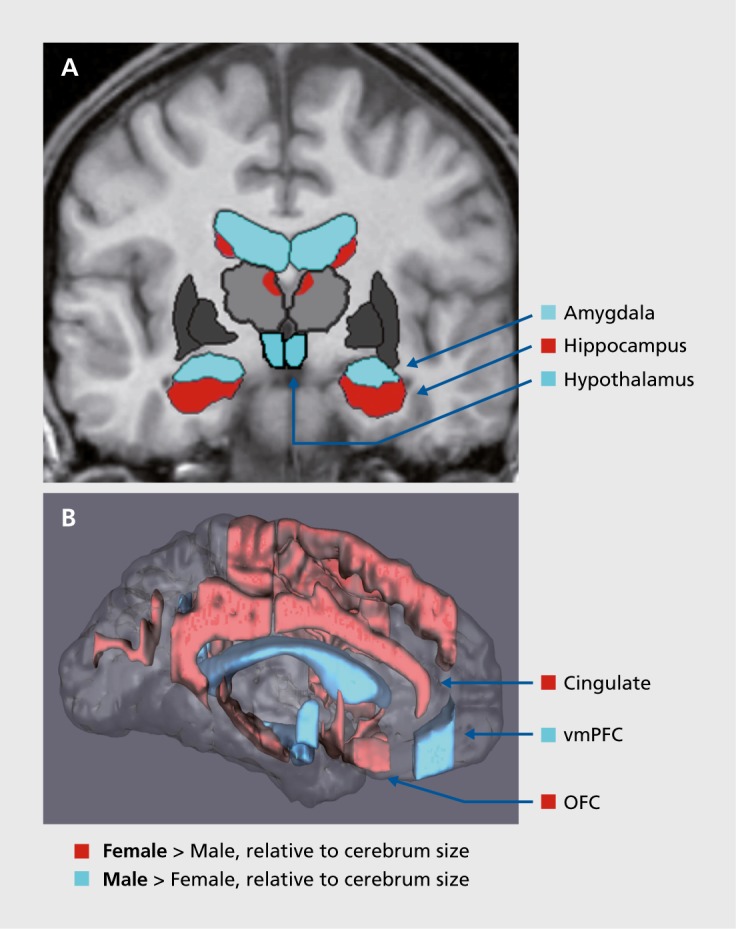
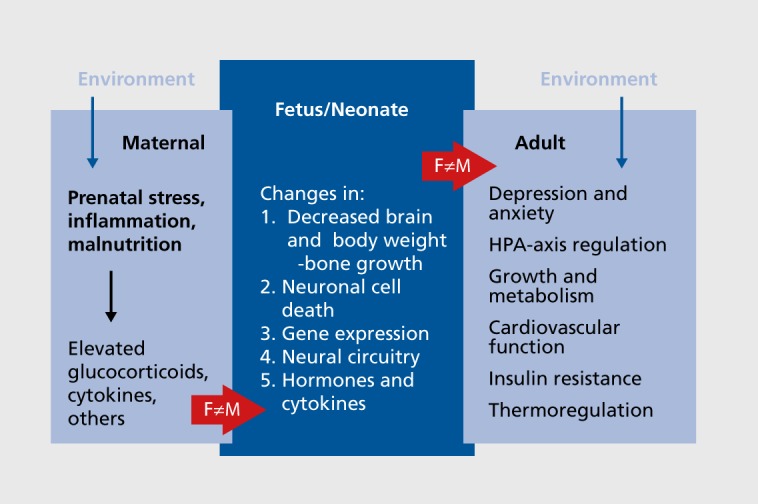
Major depressive disorder (MDD) is the number one cause of disability worldwide and is comorbid with many chronic diseases, including obesity/metabolic syndrome (MetS). Women have twice as much risk for MDD and comorbidity with obesity/MetS as men, although pathways for understanding this association remain unclear. On the basis of clinical and preclinical studies, we argue that prenatal maternal stress (ie, excess glucocorticoid expression and associated immune responses) that occurs during the sexual differentiation of the fetal brain has sex-dependent effects on brain development within highly sexually dimorphic regions that regulate mood, stress, metabolic function, the autonomic nervous system, and the vasculature. Furthermore, these effects have lifelong consequences for shared sex-dependent risk of MDD and obesity/MetS. Thus, we propose that there are shared biologic substrates at the anatomical, molecular, and/or genetic levels that produce the comorbid risk for MDD-MetS through sex-dependent fetal origins.
El trastorno depresivo mayor (TDM) es la causa número uno de incapacidad en el mundo y es comórbido con muchas enfermedades crónicas, incluyendo la obesidad y el síndrome metabólico (SMet). Si bien las mujeres tienen el doble de riesgo que los hombres para el TDM y para la comorbilidad con obesidad y SMet, aun no se han aclarado las bases para comprender esta asociación. En base a estudios clínicos y preclínicos, se argumenta que el estrés materno prenatal (como la expresión excesiva de glucocorticoides y las respuestas inmunes asociadas) que ocurre durante la diferenciación sexual del cerebro fetal tiene efectos dependientes del sexo sobre el desarrollo cerebral en las regiones con alto dimorfismo sexual que regulan el ánimo, el estrés, la función metabólica, el sistema nervioso autónomo y la vascularización. Además, estos efectos tienen consecuencias a lo largo de la vida para el riesgo compartido sexo-dependiente para TDM y obesidad/SMet. Por lo tanto, se propone que hay sustratos biológicos compartidos a niveles anatómicos, moleculares y/o genéticos que producirían el riesgo comórbido para el TDM-SMet a través de orígenes fetales sexo-dependientes.
Le trouble dépressif caractérisé (TDC) est la première cause d'invalidité dans le monde et il existe une comorbidité avec de nombreuses maladies chroniques, dont le syndrome métabolique/obésité (SMet). Le risque de TDC est deux fois plus élevé chez les femmes ayant un SMet que chez les hommes, mais les tenants et les aboutissants de cette association sont encore mal compris. Au vu des études cliniques et précliniques existantes, nous soutenons que le stress maternel prénatal (c'est-à-dire l'excès de libération de glucocorticoïdes et les réponses immunes associées) qui survient pendant la différentiation sexuelle du cerveau du foetus a des effets dépendant du sexe sur le développement cérébral dans des régions très dimorphiques sexuellement, régulant l'humeur, le stress, la fonction métabolique, le système nerveux autonome et la vascularisation. De plus, les conséquences de ces effets pour le risque partagé de TDC et de SMet/obésité en fonction du sexe durent toute la vie. Nous pensons donc qu'il existerait des substrats biologiques partagés aux niveaux anatomique, moléculaire et/ou génétique qui seraient responsables du risque comorbide de TDC-SMet selon le sexe du foetus.
Keywords: depression; depression-cardiometabolic comorbidity; fetal programming; inflammation; obesity/metabolic syndrome; prenatal stress model; sex difference.
Figures
References
-
- World Health Organization. Global health estimates 2014 summary tables: YLD by cause, age, and sex, 2000-2012. Available at: http://www. who.int/healthinfo/global_burden_disease/estimates/en/index2.html. Published June 2014. Accessed October 2016.
-
- Roberts RE., Deleger S., Strawbridge WJ., Kaplan GA. Prospective association between obesity and depression: evidence from the Alameda County Study. Int J Obes Relat Metab Disord. 2003;27(4):514–521. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical