

Prophylactic mesh placement for the PREvention of paraSTOmal hernias: The PRESTO systematic review and meta-analysis
- PMID: 28182642
- PMCID: PMC5300283
- DOI: 10.1371/journal.pone.0171548
Prophylactic mesh placement for the PREvention of paraSTOmal hernias: The PRESTO systematic review and meta-analysis
Abstract
Background: Parastomal hernia (PH) is the most common complication after ostomy formation. Prophylactic mesh placement may be effective in reducing the rate of PH at the stoma site. The aims of this systematic review were to summarize the evidence with regard to the safety and effectiveness in comparison with the standard procedure without mesh placement and to identify important risk constellations.
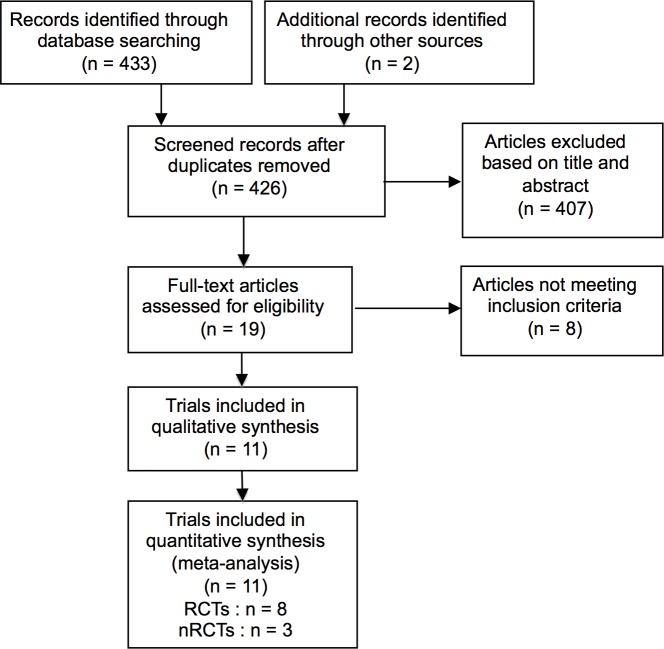
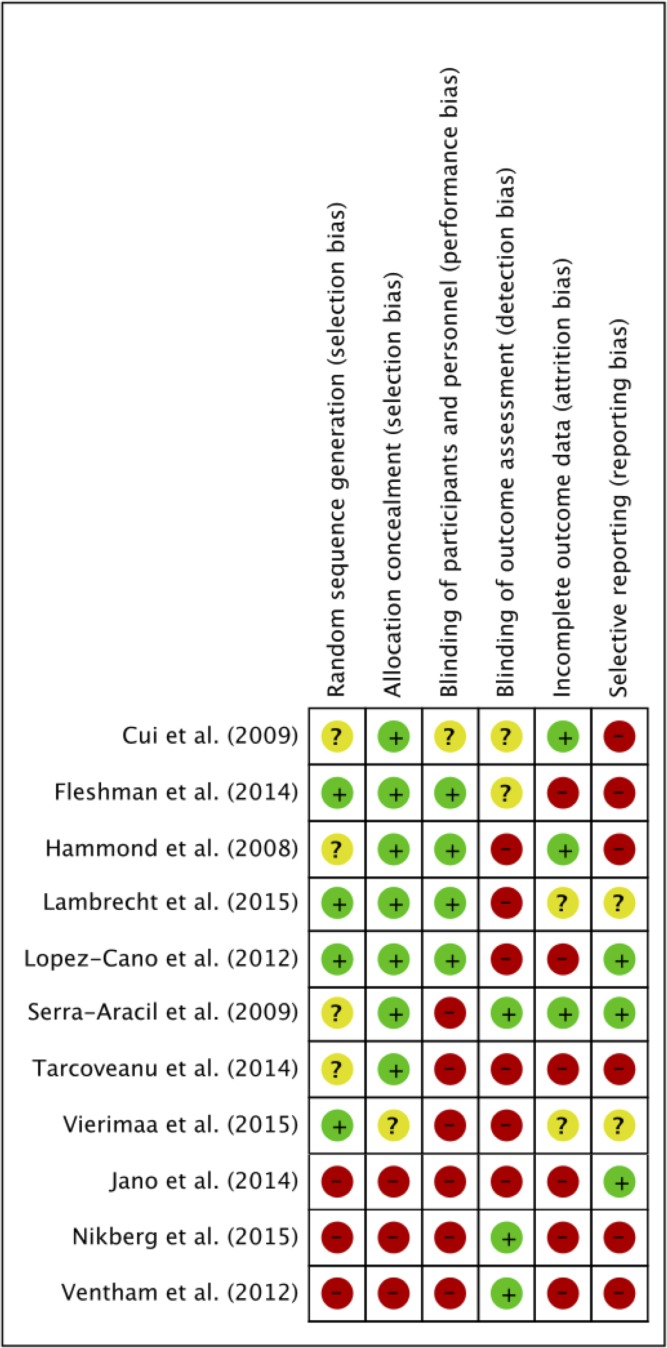
Method: A systematic literature search was performed in PubMed, EMBASE and the Cochrane library with no language or date restrictions. Randomized (RCTs) and non-randomized controlled trials (nRCTs) were included. The main outcomes of interest were PH (primary outcome) rate and stoma-related complications (secondary outcomes) such as stenosis or fistula. Statistical analysis included meta-analyses of pooled data and subgroup analyses.
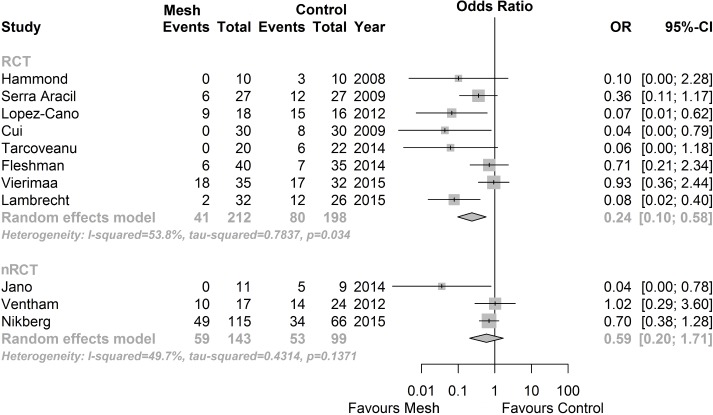
Results: Eleven trials (eight RCTs; three nRCTs) with a total of 755 patients were included. PH rate varied from 0% to 59% in the intervention and from 20% to 94% in the control group. RCTs showed a significant reduction of PH rate in the mesh group (OR 0.24; 95% CI 0.10 to 0.58, p = 0.034), whereas included nRCTs did not. No significant differences were observed in postoperative complication rates. Subgroup analyses showed superiority of non-absorbable meshes and sublay mesh positioning in open surgery.
Conclusion: Prophylactic mesh placement is safe and reduces PH rate. A recommendation for prophylactic non-absorbable meshes in a sublay position can be made for patients undergoing open colorectal operations with end-ostomies. Further research endeavors should focus on patient-oriented outcomes, not only PH rate, with respect to tailored treatment in specific patient populations.
Conflict of interest statement
The authors have declared that no competing interests exist.
Figures
References
-
- Pearl RK. Parastomal hernias. World journal of surgery. 1989;13(5):569–72. - PubMed
-
- Helgstrand F, Gogenur I, Rosenberg J. Prevention of parastomal hernia by the placement of a mesh at the primary operation. Hernia: the journal of hernias and abdominal wall surgery. 2008;12(6):577–82. Epub 2008/06/05. - PubMed
-
- Allen-Mersh TG, Thomson JP. Surgical treatment of colostomy complications. The British journal of surgery. 1988;75(5):416–8. - PubMed
-
- Cheung MT. Complications of an abdominal stoma: an analysis of 322 stomas. The Australian and New Zealand journal of surgery. 1995;65(11):808–11. - PubMed
-
- Sakai Y, Nelson H, Larson D, Maidl L, Young-Fadok T, Ilstrup D. Temporary transverse colostomy vs loop ileostomy in diversion: a case-matched study. Archives of surgery. 2001;136(3):338–42. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
