

Impact of dexmedetomidine on the incidence of delirium in elderly patients after cardiac surgery: A randomized controlled trial
- PMID: 28182690
- PMCID: PMC5300174
- DOI: 10.1371/journal.pone.0170757
Impact of dexmedetomidine on the incidence of delirium in elderly patients after cardiac surgery: A randomized controlled trial
Abstract
Background: Delirium is a frequent complication after cardiac surgery and its occurrence is associated with poor outcomes. The purpose of this study was to investigate the impact of perioperative dexmedetomidine administration on the incidence of delirium in elderly patients after cardiac surgery.
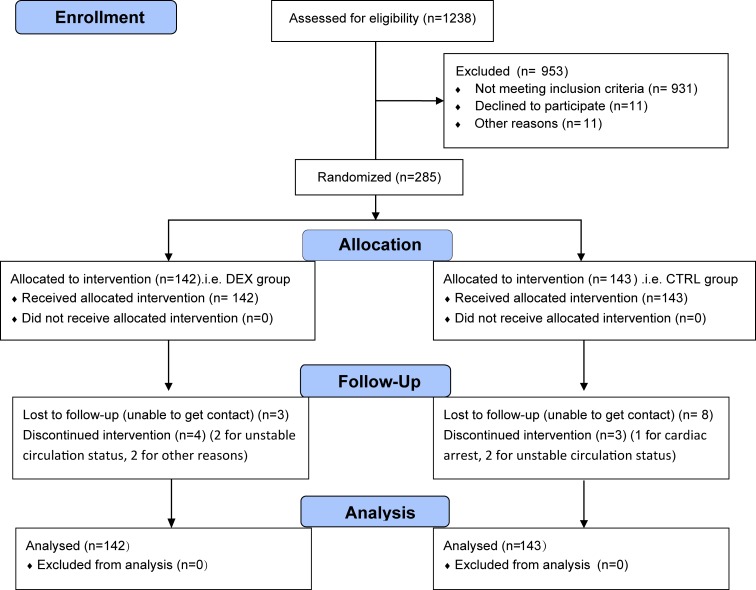
Methods: This randomized, double-blinded, and placebo-controlled trial was conducted in two tertiary hospitals in Beijing between December 1, 2014 and July 19, 2015. Eligible patients were randomized into two groups. Dexmedetomidine (DEX) was administered during anesthesia and early postoperative period for patients in the DEX group, whereas normal saline was administered in the same rate for the same duration for patients in the control (CTRL) group. The primary endpoint was the incidence of delirium during the first five days after surgery. Secondary endpoints included the cognitive function assessed on postoperative days 6 and 30, the overall incidence of non-delirium complications within 30 days after surgery, and the all-cause 30-day mortality.
Results: Two hundred eighty-five patients were enrolled and randomized. Dexmedetomidine did not decrease the incidence of delirium (4.9% [7/142] in the DEX group vs 7.7% [11/143] in the CTRL group; OR 0.62, 95% CI 0.23 to 1.65, p = 0.341). Secondary endpoints were similar between the two groups; however, the incidence of pulmonary complications was slightly decreased (OR 0.51, 95% CI 0.26 to 1.00, p = 0.050) and the percentage of early extubation was significantly increased (OR 3.32, 95% CI 1.36 to 8.08, p = 0.008) in the DEX group. Dexmedetomidine decreased the required treatment for intraoperative tachycardia (21.1% [30/142] in the DEX group vs 33.6% [48/143] in the CTRL group, p = 0.019), but increased the required treatment for postoperative hypotension (84.5% [120/142] in the DEX group vs 69.9% [100/143] in the CTRL group, p = 0.003).
Conclusions: Dexmedetomidine administered during anesthesia and early postoperative period did not decrease the incidence of postoperative delirium in elderly patients undergoing elective cardiac surgery. However, considering the low delirium incidence, the trial might have been underpowered.
Trial registration: ClinicalTrials.gov NCT02267538.
Conflict of interest statement
Dr DX Wang received lecture fees and/or travel expenses for lectures given at domestic academic meetings from Jiangsu Hengrui Medicine Co., Ltd., China. Prof D Ma is supported by BOC Chair grant, Royal College of Anaesthetists, and BJA Fellowship grant, London, UK. Other authors reported no conflict of interests. These does not alter our adherence to PLOS ONE policies on sharing data and materials.
Figures
References
-
- Koster S, Hensens AG, van der Palen J. The long-term cognitive and functional outcomes of postoperative delirium after cardiac surgery. Ann Thoric Surg 2009, 87(5):1469–1474. - PubMed
-
- Radtke FM, Franck M, Lendner J, Kruger S, Wernecke KD, Spies CD. Monitoring depth of anaesthesia in a randomized trial decreases the rate of postoperative delirium but not postoperative cognitive dysfunction. Br J Anaesth 2013, 110 Suppl 1:i98–i105. - PubMed
