

Kidney function and specific mortality in 60-80 years old post-myocardial infarction patients: A 10-year follow-up study
- PMID: 28182761
- PMCID: PMC5300181
- DOI: 10.1371/journal.pone.0171868
Kidney function and specific mortality in 60-80 years old post-myocardial infarction patients: A 10-year follow-up study
Abstract
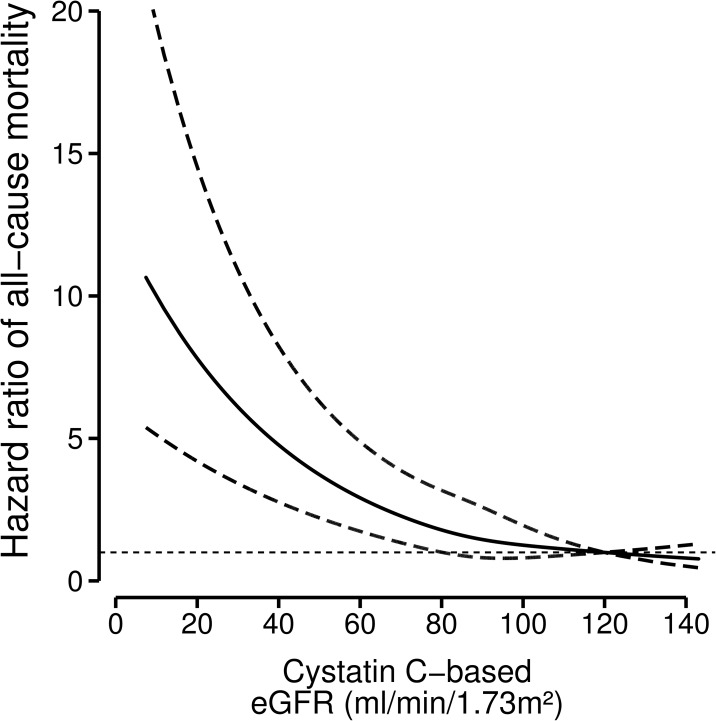
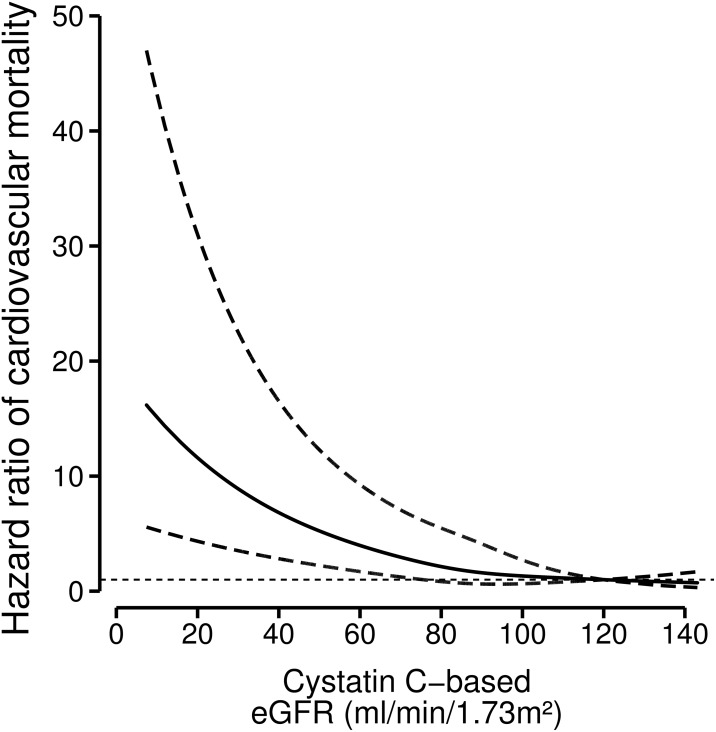
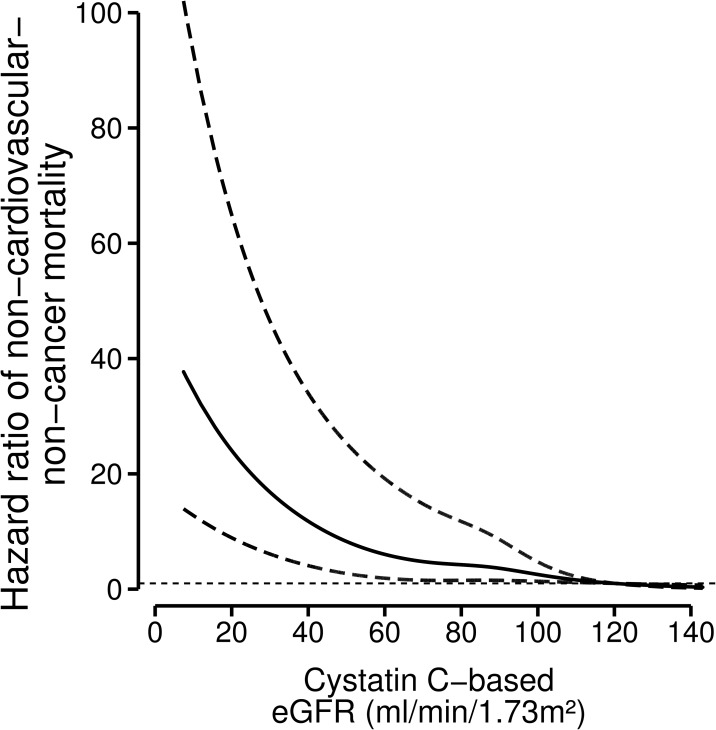
Chronic kidney disease (CKD) is highly prevalent among older post-myocardial infarction (MI) patients. It is not known whether CKD is an independent risk factor for mortality in older post-MI patients with optimal cardiovascular drug-treatment. Therefore, we studied the relation between kidney function and all-cause and specific mortality among older post-MI patients, without severe heart failure, who are treated with state-of-the-art pharmacotherapy. From 2002-2006, 4,561 Dutch post-MI patients were enrolled and followed until death or January 2012. We estimated Glomerular Filtration Rate (eGFR) with cystatin C (cysC) and creatinine (cr) using the CKD-EPI equations and analyzed the relation with any and major causes of death using Cox models and restricted cubic splines. Mean (SD) for age was 69 years (5.6), 79% were men, 17% smoked, 21% had diabetes, 90% used antihypertensive drugs, 98% used antithrombotic drugs and 85% used statins. Patients were divided into four categories of baseline eGFRcysC: ≥90 (33%; reference), 60-89 (47%), 30-59 (18%), and <30 (2%) ml/min/1.73m2. Median follow-up was 6.4 years. During follow-up, 873 (19%) patients died: 370 (42%) from cardiovascular causes, 309 (35%) from cancer, and 194 (22%) from other causes. After adjustment for age, sex and classic cardiovascular risk factor, hazard ratios (95%-confidence intervals) for any death according to the four eGFRcysC categories were: 1 (reference), 1.4 (1.1-1.7), 2.9 (2.3-3.6) and 4.4 (3.0-6.4). The hazard ratios of all-cause and cause-specific mortality increased linearly below kidney functions of 80 ml/min/1.73 m2. Weaker results were obtained for eGFRcr. To conclude, we found in optimal cardiovascular drug-treated post-MI patients an inverse graded relation between kidney function and mortality for both cardiovascular as well as non-cardiovascular causes. Risk of mortality increased linearly below kidney function of about 80 ml/min/1.73 m2.
Conflict of interest statement
The authors have declared that no competing interests exist.
Figures
References
-
- Lindeman RD, Tobin J, Shock NW. Longitudinal studies on the rate of decline in renal function with age. J Am Geriatr Soc. 1985;33: 278–285. - PubMed
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
