

Towards an optimal therapy strategy for myogenous TMD, physiotherapy compared with occlusal splint therapy in an RCT with therapy-and-patient-specific treatment durations
- PMID: 28183288
- PMCID: PMC5301345
- DOI: 10.1186/s12891-017-1404-9
Towards an optimal therapy strategy for myogenous TMD, physiotherapy compared with occlusal splint therapy in an RCT with therapy-and-patient-specific treatment durations
Abstract
Background: Temporomandibular Disorders (TMD) may be characterized by pain and restricted jaw movements. In the absence of somatic factors in the temporomandibular joint, mainly myogenous, psychobiological, and psychosocial factors may be involved in the aetiology of myogenous TMD. An occlusal appliance (splint) is commonly used as a basic therapy of the dental practice. Alternatively, a type of physiotherapy which includes, apart from massage of sore muscles, aspects of cognitive-behavioural therapy might be a basic therapy for myogenous TMD. Treatment outcome of physiotherapy (Ph-Tx) was evaluated in comparison to that of splint therapy (Sp-Tx), using the index Treatment Duration Control (TDC) that enabled a randomized controlled trial with, comparable to clinical care, therapy-and-patient-specific treatment durations.
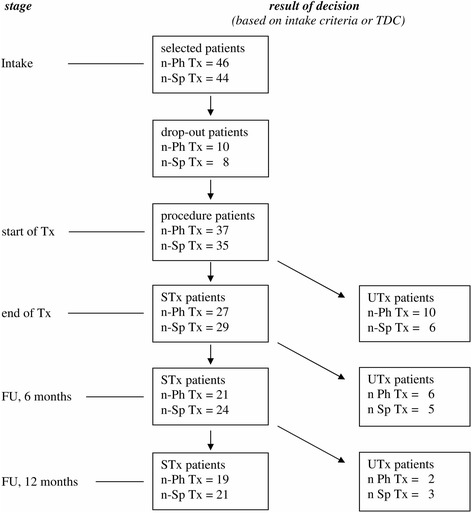
Methods: Seventy-two patients were randomly assigned to either Ph-Tx or Sp-Tx, with an intended treatment duration between 10 and 21 or 12 and 30 weeks respectively. Using TDC, the clinician controlled treatment duration and the number of visits needed. A blinded assessor recorded anamnestic and clinical data to determine TDC-values following treatment and a 1-year follow-up, yielding success rate (SR) and effectiveness (mean TDC) as treatment outcomes. Cohen's d, was determined for pain intensity. Overall SR for stepped-care was assessed in a theoretical model, i.e. a second of the two studied therapies was applied if the first treatment was unsuccessful, and the effect of therapy sequence and difference in success rates was examined.
Results: SR and effectiveness were similar for Ph-Tx and Sp-Tx (long-term SR: 51-60%; TDC: -0.512- -0.575). Cohen's d was 0.86 (Ph-Tx) and 1.39 (Sp-Tx). Treatment duration was shorter for Ph-Tx (on average 10.4 weeks less; p < 0.001). Sp-Tx needed 7.1 less visits (p < 0.001).
Conclusions: Physiotherapy may be preferred as initial therapy over occlusal splint therapy in stepped-care of myogenous TMD. With a similar SR and effectiveness, physiotherapy has a shorter duration. Thus patients whose initial physiotherapy is unsuccessful can continue earlier with subsequent treatment. The stepped-care model reinforces the conclusion on therapy preference as the overall SR hardly depends on therapy sequence.
Trial registration: isrctn.com/ISRCTN17469828 . Retrospectively registered: 11/11/2016.
Keywords: Medical decision; Myofascial pain syndrome; Occlusal splint; Physiotherapy; Randomized controlled trial; Stepped-care; Temporomandibular disorders.
Figures

References
-
- Okeson JP. Orofacial pain: guidelines for assessment, classification, and management. The American Academy of Orofacial Pain. Illinois: Quintessence; 1996.
-
- Dworkin SF, LeResche L. Research diagnostic criteria for temporomandibular mandibular disorders: review, criteria, examinations and specifications, critique. J Craniomandib Disord. 1992;6:301–355. - PubMed
-
- Benoliel R, Svensson P, Eliav E. Pathophysiology of masticatory myofascial pain. In: Greene CS, Laskin DM, editors. Treatment of TMDs: bridging the gap between advances in research and clinical patient management. Illinois: Quintessence; 2013. pp. 17–32.
-
- Dubner R, Ren K, Sessle BJ. Sensory mechanisms of orofacial pain. In: Greene CS, Laskin DM, editors. Treatment of TMDs: bridging the gap between advances in research and clinical patient management. Illinois: Quintessence; 2013. pp. 3–16.
Publication types
MeSH terms
Associated data
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
