

Prevalence and associated factors of resting electrocardiogram abnormalities among systemic lupus erythematosus patients without cardiovascular disease
- PMID: 28183339
- PMCID: PMC5301322
- DOI: 10.1186/s13075-017-1240-1
Prevalence and associated factors of resting electrocardiogram abnormalities among systemic lupus erythematosus patients without cardiovascular disease
Abstract
Background: Electrocardiogram (ECG) cardiovascular disease (CVD) abnormalities (ECG-CVD) are predictive of subsequent CVD events in the general population. Systemic lupus erythematosus (SLE) patients are vulnerable to CVD. We aimed to determine the prevalence of ECG-CVD in SLE patients and to examine the risk factors associated with ECG-CVD.
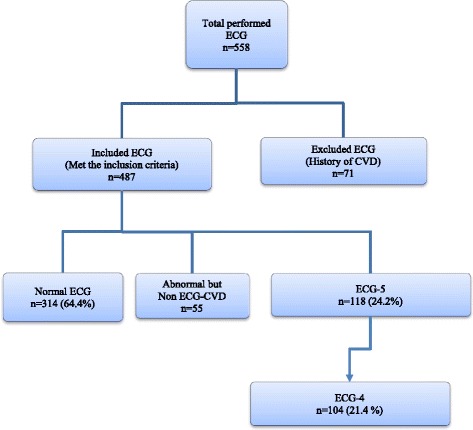
Methods: A 12-lead resting supine ECG was performed on consecutive adult patients attending the clinic. One cardiologist interpreted the ECGs. ECG-CVD were defined as the presence of one or more of the following 4 elements (ECG-4): ST-segment and/or T-wave abnormalities, left ventricular hypertrophy (LVH), left axis deviation (LAD), left bundle branch block (LBBB) and right bundle branch block (RBBB). ECG-5 included the same elements as ECG-4 and the Q-wave. Repeated measurement data were created and the associations between ECG-4/ECG-5 and demographics were evaluated with univariate and multivariate Cox regression models.
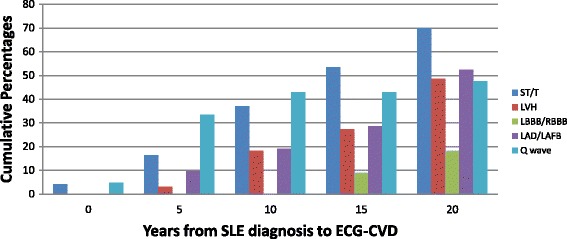
Results: Of 487 SLE patients, 104 (21.4%) and 118 (24.2%) patients had one or more of the ECG-4 and ECG-5 elements, respectively. A higher prevalence of ECG-CVD was found in patients with a longer SLE disease duration, and the burden of ECG-CVD elements increased with age. Increased age, active SLE disease, and damage were associated with ECG4 and ECG-5, while treatment of hyperlipidemia was protective.
Conclusion: A high prevalence of ECG-4 (21.4%) and ECG-5 (24.2%) was found in this SLE cohort. Controlling SLE disease activity is important since it was associated with ECG-4 and ECG-5. Early identification of ECG-4 and ECG-5 in SLE patients might allow for better stratification and risk management.
Keywords: Cardiovascular disease; Electrocardiogram; Systemic lupus erythematosus.
Figures
References
-
- Gladman DD, Urowitz MB. Morbidity in systemic lupus erythematosus. J Rheumatol Suppl. 1987;14(Suppl 13):223–6. - PubMed
-
- Urowitz MB, Ibanez D, Gladman DD. Atherosclerotic vascular events in a single large lupus cohort: prevalence and risk factors. J Rheumatol. 2007;34(1):70–5. - PubMed
-
- Abu-Shakra M, Urowitz MB, Gladman DD, Gough J. Mortality studies in systemic lupus erythematosus. Results from a single center. II. Predictor variables for mortality. J Rheumatol. 1995;22(7):1265–70. - PubMed
-
- Manzi S, Meilahn EN, Rairie JE, Conte CG, Medsger TA, Jr, Jansen-McWilliams L, et al. Age-specific incidence rates of myocardial infarction and angina in women with systemic lupus erythematosus: comparison with the Framingham Study. Am J Epidemiol. 1997;145(5):408–15. doi: 10.1093/oxfordjournals.aje.a009122. - DOI - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
