

FACTORS ASSOCIATED WITH WOMEN'S HEALTH CARE DECISION-MAKING AUTONOMY: EMPIRICAL EVIDENCE FROM NIGERIA
- PMID: 28183370
- PMCID: PMC6010313
- DOI: 10.1017/S0021932017000037
FACTORS ASSOCIATED WITH WOMEN'S HEALTH CARE DECISION-MAKING AUTONOMY: EMPIRICAL EVIDENCE FROM NIGERIA
Abstract
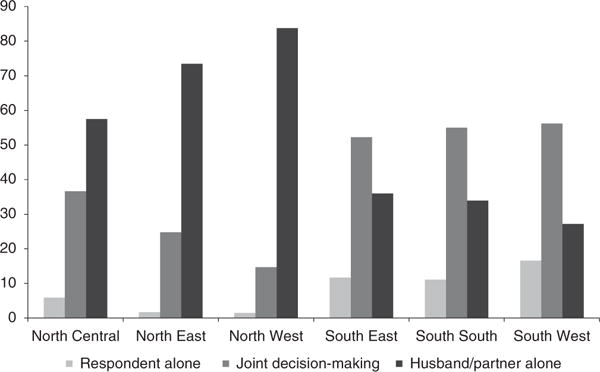
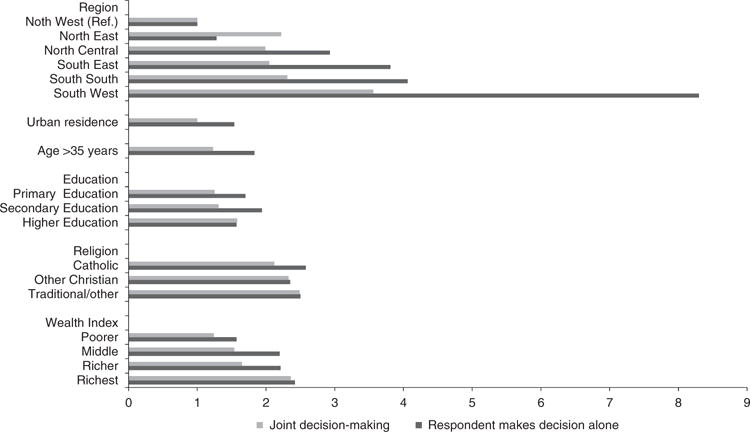
Women's decision-making autonomy has been poorly studied in most developing countries. The few existing studies suggest that it is closely linked to women's socio-demographic characteristics and the social settings in which they live. This study examined Nigerian women's perceived decision-making autonomy about their own health care using nationally representative data from the 2013 Nigerian Demographic and Health Survey. The study sample consisted of 27,135 women aged 15-49 years who lived with their husbands/partners. Responses to questions about who usually makes decisions about the respondent's health care were analysed. Factors associated with women's health care decision-making were investigated using logistic regression models. Only 6.2% of the women reported making their own decisions about health care. For most women (61.1%), this decision was made by their husband/partner alone and 32.7% reported joint decision-making with their husband/partner. Factors independently associated with decision-making by the woman included: geographical region, rural/urban residence, age, education, religion, wealth index, occupation, home ownership and husband's occupation. A strong association between women making their own health care decision was seen with region of residence (χ 2=3221.48, p<0.0001), even after controlling for other factors. Notably, women from the South West region were 8.3 times more likely to make their own health care decisions than women from the North West region. Factors that were significantly associated with joint health care decision-making were also significantly associated with decision-making by the woman alone. The study found that individual-level factors were significantly associated with Nigerian women's decision-making autonomy, as well as other factors, in particular geographic region. The findings provide an important perspective on women's health care decision-making autonomy in a developing country.
Conflict of interest statement
The authors have no conflicts of interest to declare.
Figures
References
-
- Al Riyami A, Afifi M, Mabry RM. Women’s autonomy, education and employment in Oman and their influence on contraceptive use. Reproductive Health Matters. 2004;12:144–154. - PubMed
-
- Balk D. Individual and community aspects of women’s status and fertility in rural Bangladesh. Population Studies. 1994;48(1):21–45.
-
- Basu AM. Culture, the Status of Women, and Demographic Behaviour: Illustrated with the Case of India. Clarendon Press; Oxford: 1992.
-
- Becker S, Fonseca-Becker F, Schenck-Yglesias C. Husbands’ and wives’ reports of women’s decision-making power in Western Guatemala and their effects on preventive health behaviours. Social Science & Medicine. 2006;62:2313–2326. - PubMed
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
