

Autoimmune Encephalitis: Pathophysiology and Imaging Review of an Overlooked Diagnosis
- PMID: 28183838
- PMCID: PMC7960083
- DOI: 10.3174/ajnr.A5086
Autoimmune Encephalitis: Pathophysiology and Imaging Review of an Overlooked Diagnosis
Abstract
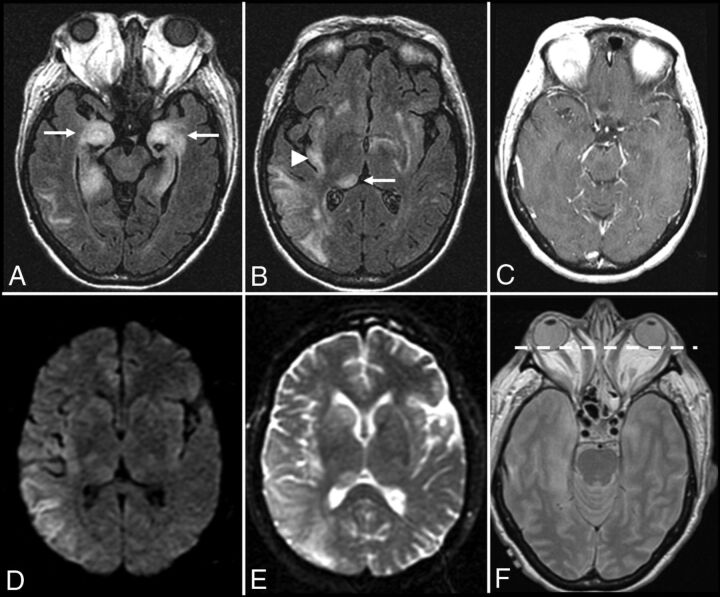
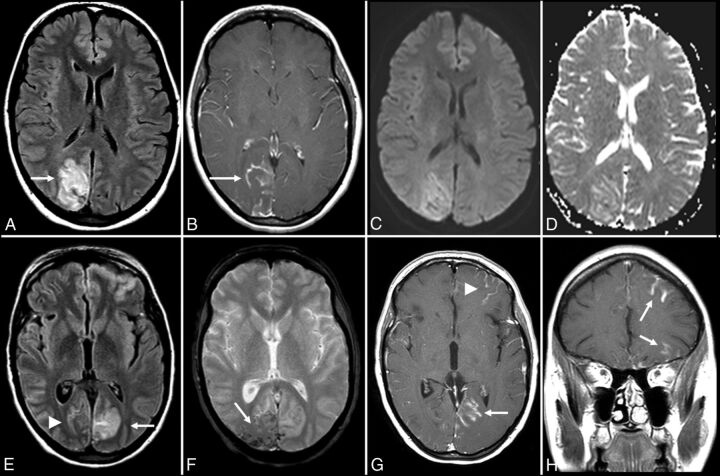
Autoimmune encephalitis is a relatively new category of immune-mediated disease involving the central nervous system that demonstrates a widely variable spectrum of clinical presentations, ranging from the relatively mild or insidious onset of cognitive impairment to more complex forms of encephalopathy with refractory seizure. Due to its diverse clinical features, which can mimic a variety of other pathologic processes, autoimmune encephalitis presents a diagnostic challenge to clinicians. Imaging findings in patients with these disorders can also be quite variable, but recognizing characteristic findings within limbic structures suggestive of autoimmune encephalitis can be a key step in alerting clinicians to the potential diagnosis and ensuring a prompt and appropriate clinical work-up. In this article, we review antibody-mediated encephalitis and its various subtypes with a specific emphasis on the role of neuroimaging in the diagnostic work-up.
© 2017 by American Journal of Neuroradiology.
Figures





References
Publication types
MeSH terms
Supplementary concepts
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical