

Decreased Diastolic Ventricular Kinetic Energy in Young Patients with Fontan Circulation Demonstrated by Four-Dimensional Cardiac Magnetic Resonance Imaging
- PMID: 28184976
- PMCID: PMC5388704
- DOI: 10.1007/s00246-016-1565-6
Decreased Diastolic Ventricular Kinetic Energy in Young Patients with Fontan Circulation Demonstrated by Four-Dimensional Cardiac Magnetic Resonance Imaging
Erratum in
-
Erratum to: Decreased Diastolic Ventricular Kinetic Energy in Young Patients with Fontan Circulation Demonstrated by Four-Dimensional Cardiac Magnetic Resonance Imaging.Pediatr Cardiol. 2017 Jun;38(5):1087. doi: 10.1007/s00246-017-1617-6. Pediatr Cardiol. 2017. PMID: 28456830 Free PMC article. No abstract available.
Abstract
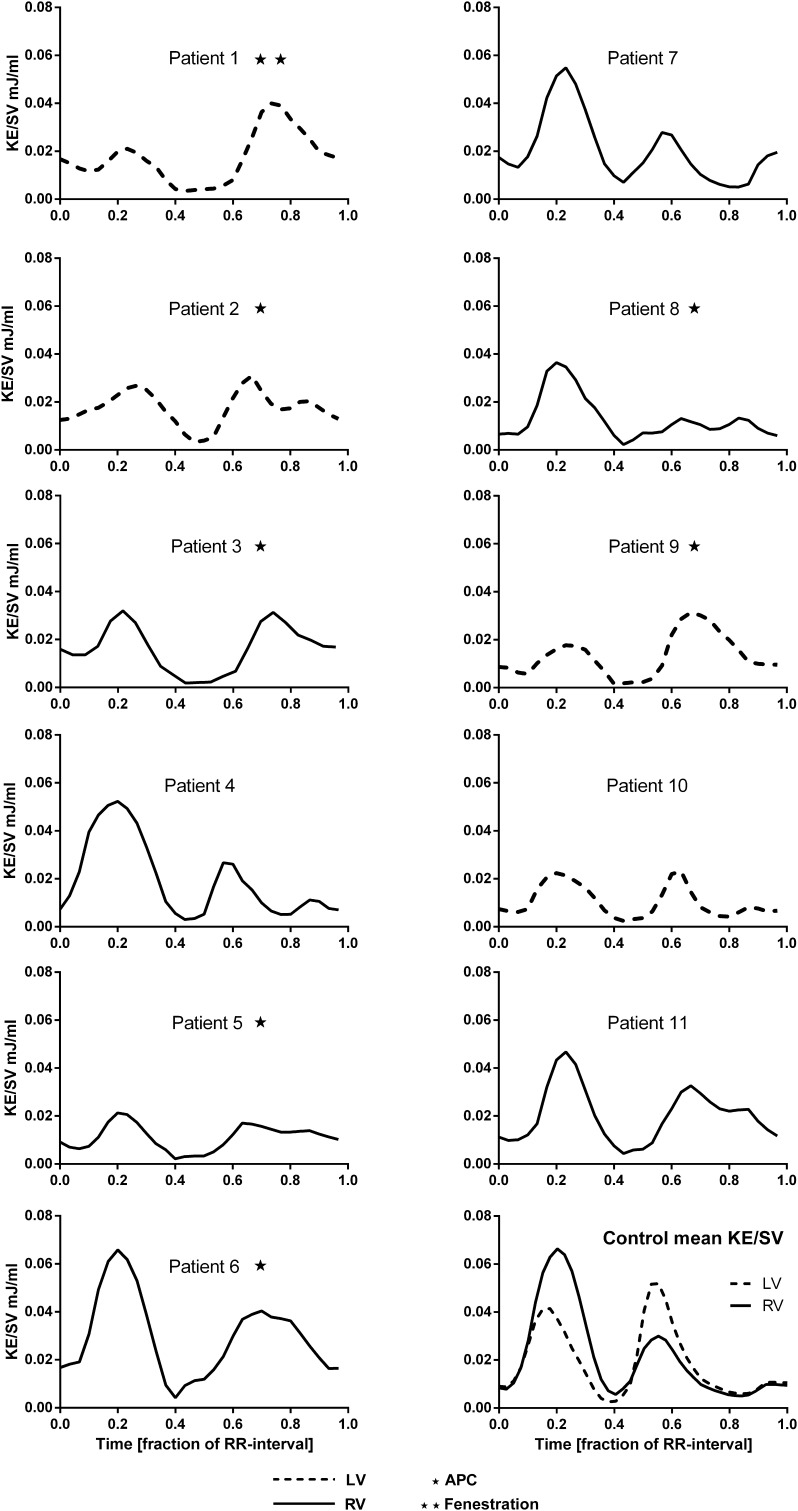
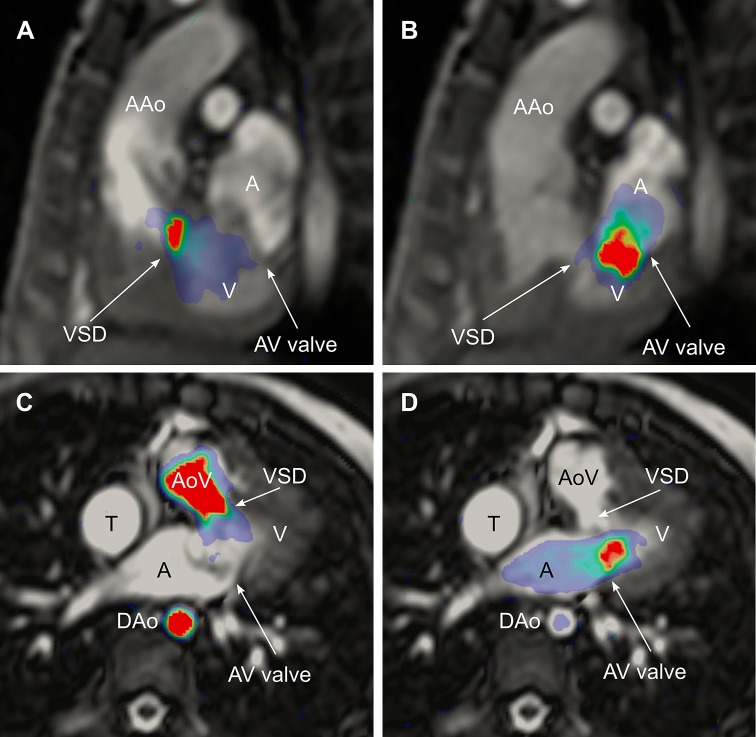
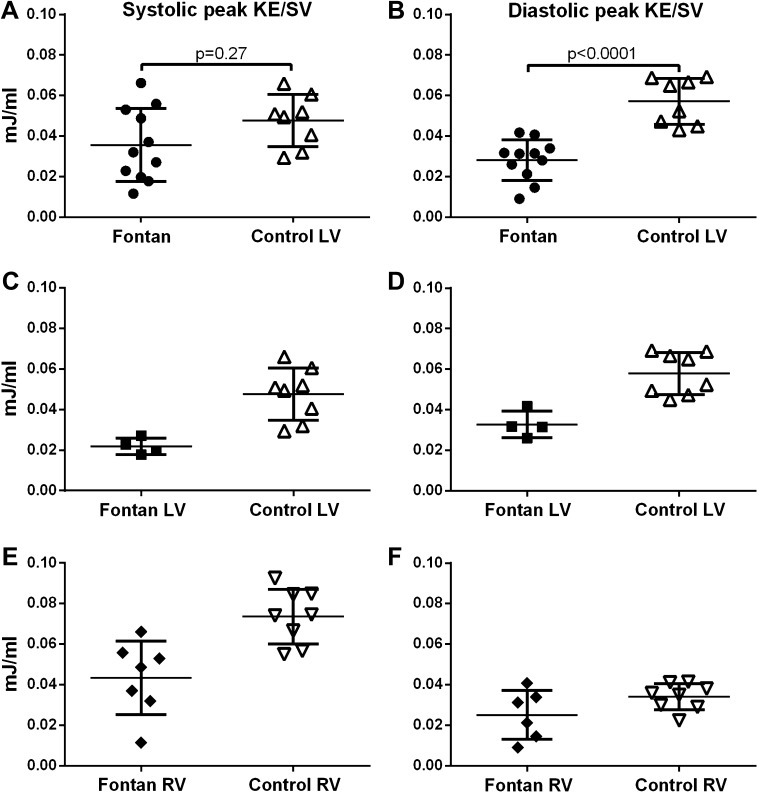
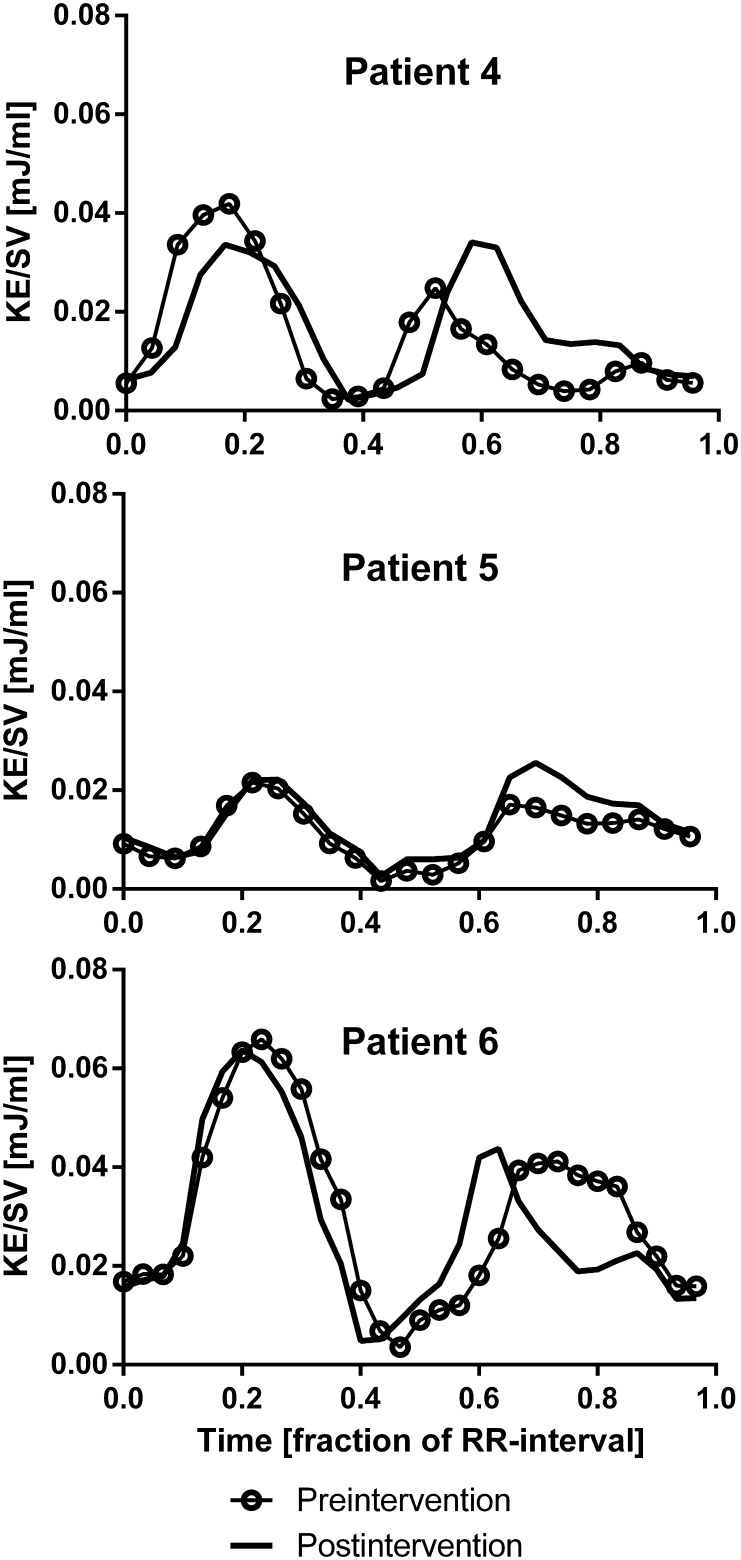
Four-dimensional (4D) flow magnetic resonance imaging (MRI) enables quantification of kinetic energy (KE) in intraventricular blood flow. This provides a novel way to understand the cardiovascular physiology of the Fontan circulation. In this study, we aimed to quantify the KE in functional single ventricles. 4D flow MRI was acquired in eleven patients with Fontan circulation (median age 12 years, range 3-29) and eight healthy volunteers (median age 26 years, range 23-36). Follow-up MRI after surgical or percutaneous intervention was performed in 3 patients. Intraventricular KE was calculated throughout the cardiac cycle and indexed to stroke volume (SV). The systolic/diastolic ratio of KE in Fontan patients was similar to the ratio of the controls' left ventricle (LV) or right ventricle (RV) depending on the patients' ventricular morphology (Cohen´s κ = 1.0). Peak systolic KE/SV did not differ in patients compared to the LV in controls (0.016 ± 0.006 mJ/ml vs 0.020 ± 0.004 mJ/ml, p = 0.09). Peak diastolic KE/SV in Fontan patients was lower than in the LV of the control group (0.028 ± 0.010 mJ/ml vs 0.057 ± 0.011 mJ/ml, p < 0.0001). The KE during diastole showed a plateau in patients with aortopulmonary collaterals. This is to our knowledge the first study that quantifies the intraventricular KE of Fontan patients. KE is dependent on the morphology of the ventricle, and diastolic KE indexed to SV in patients is decreased compared to controls. The lower KE in Fontan patients may be a result of impaired ventricular filling.
Keywords: CMR; Congenital heart disease; Fontan; Kinetic energy; MRI; Magnetic resonance imaging.
Conflict of interest statement
Einar Heiberg is stockholder and founder of the medical image analysis company Medviso AB that sells the Segment software for clinical use. Hakan Arheden is stockholder of Imacor AB, a core lab for medical image analysis. Marcus Carlsson has received consultancy fees from Imacor AB. The remaining authors have no disclosures.
Figures
References
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
