

Safety and feasibility of minimally invasive gastrectomy during the early introduction in the Netherlands: short-term oncological outcomes comparable to open gastrectomy
- PMID: 28185027
- PMCID: PMC5569663
- DOI: 10.1007/s10120-017-0695-8
Safety and feasibility of minimally invasive gastrectomy during the early introduction in the Netherlands: short-term oncological outcomes comparable to open gastrectomy
Abstract
Background: Minimally invasive techniques for gastric cancer surgery have recently been introduced in the Netherlands, based on a proctoring program. The aim of this population-based cohort study was to evaluate the short-term oncological outcomes of minimally invasive gastrectomy (MIG) during its introduction in the Netherlands.
Methods: The Netherlands Cancer Registry identified all patients with gastric adenocarcinoma who underwent gastrectomy with curative intent between 2010 and 2014. Multivariable analysis was performed to compare MIG and open gastrectomy (OG) on lymph node yield (≥15), R0 resection rate, and 1-year overall survival. The pooled learning curve per center of MIG was evaluated by groups of five subsequent procedures.
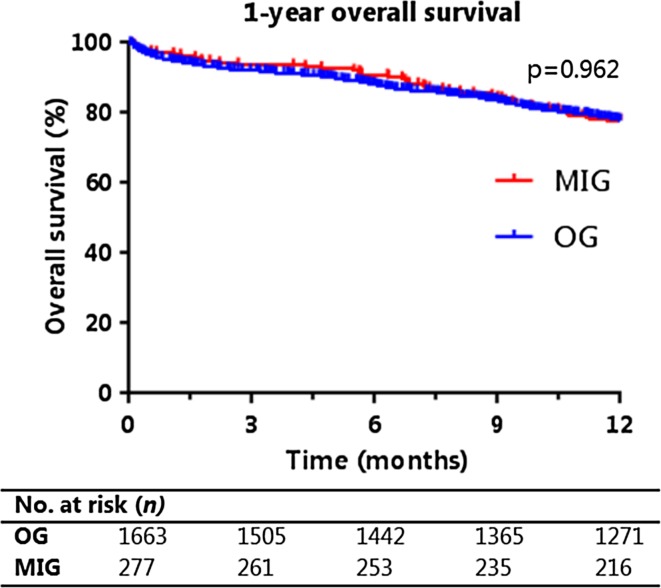
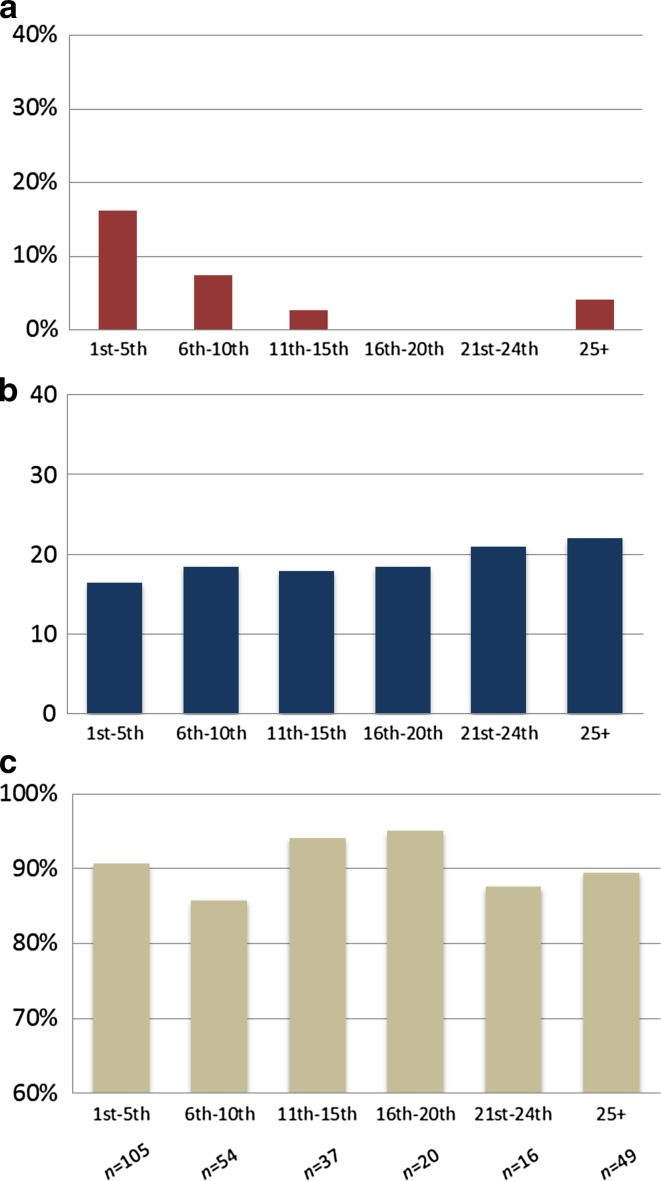
Results: Between 2010 and 2014, a total of 277 (14%) patients underwent MIG and 1633 (86%) patients underwent OG. During this period, the use of MIG and neoadjuvant chemotherapy increased from 4% to 39% (p < 0.001) and from 47% to 62% (p < 0.001), respectively. The median lymph node yield increased from 12 to 20 (p < 0.001), and the R0 resection rate remained stable, from 86% to 91% (p = 0.080). MIG and OG had a comparable lymph node yield (OR, 1.01; 95% CI, 0.75-1.36), R0 resection rate (OR, 0.86; 95% CI, 0.54-1.37), and 1-year overall survival (HR, 0.99; 95% CI, 0.75-1.32). A pooled learning curve of ten procedures was demonstrated for MIG, after which the conversion rate (13%-2%; p = 0.001) and lymph node yield were at a desired level (18-21; p = 0.045).
Conclusion: With a proctoring program, the introduction of minimally invasive gastrectomy in Western countries is feasible and can be performed safely.
Keywords: Gastric cancer; Learning curve; Lymph nodes; Minimally invasive; Survival.
Conflict of interest statement
Conflict of interest
H.J.F. Brenkman, J.P. Ruurda, R.H. Verhoeven, and R. van Hillegersberg have no conflicts of interest or financial ties to disclose.
Human rights statement and informed consent
All procedures followed were in accordance with the ethical standards of the responsible committee on human experimentation (institutional and national) and with the Helsinki Declaration of 1964 and later versions. This study was performed with nationwide, anonymous data; thus, informed consent or substitute for it was waived by the ethical review board of the NCR.
Figures

References
-
- Kitano S, Iso Y, Moriyama M, Sugimachi K. Laparoscopy-assisted Billroth I gastrectomy. Surg Laparosc Endosc. 1994;4:146–148. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
