

Role of the Gut on Glucose Homeostasis: Lesson Learned from Metabolic Surgery
- PMID: 28185153
- PMCID: PMC5306308
- DOI: 10.1007/s11883-017-0642-5
Role of the Gut on Glucose Homeostasis: Lesson Learned from Metabolic Surgery
Abstract
Purpose of review: Bariatric surgery was initially intended to reduce weight, and only subsequently was the remission of type two diabetes (T2D) observed as a collateral event. At the moment, the term "metabolic surgery" is used to underline the fact that this type of surgery is performed specifically to treat diabetes and its metabolic complications, such as hyperlipidemia.
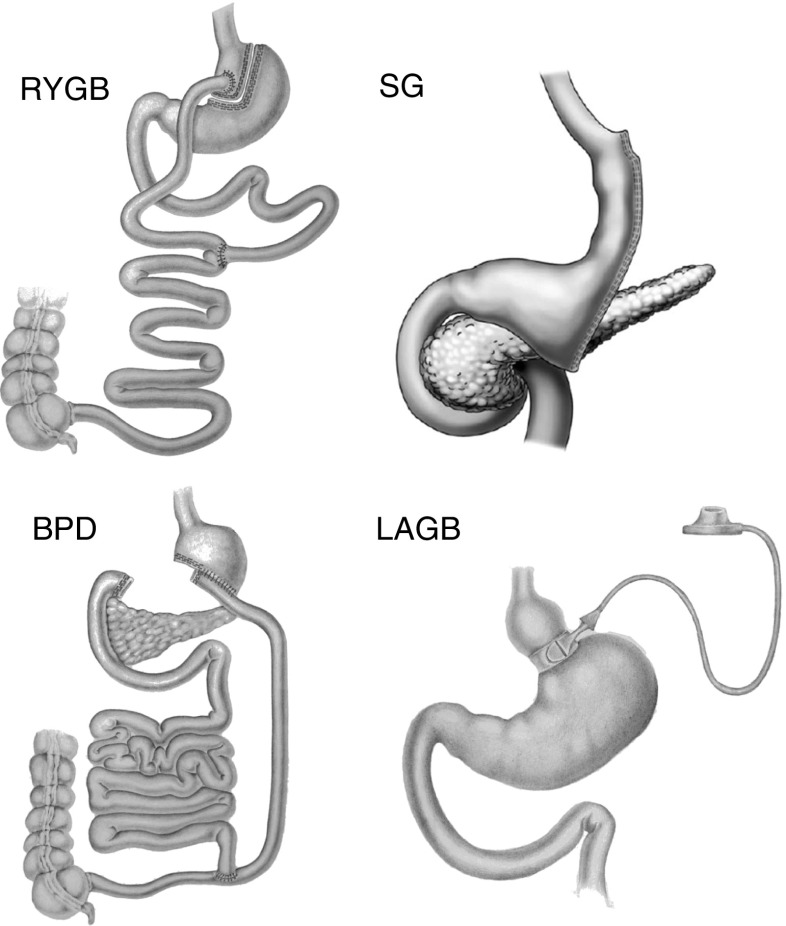
Recent findings: Randomized, controlled studies have recently supported the use of bariatric surgery, and in particular of Roux-en-Y gastric bypass (RYGB) and biliopancreatic diversion (BPD) as an effective treatment for decompensated T2D. The lesson learned from these randomized and many other non-randomized clinical studies is that the stomach and the small intestine play a central role in glucose homeostasis. Bypassing the duodenum and parts of the jejunum exerts a substantial effect on insulin sensitivity and secretion. In fact, with BPD, nutrient transit bypasses duodenum, the entire jejunum and a small portion of the ileum, resulting in reversal of insulin sensitivity back to normal and reduction of insulin secretion, whereas RYGB has little effect on insulin resistance but increases insulin secretion. Hypotheses concerning the mechanism of action of metabolic surgery for diabetes remission vary from theories focusing on jejunal nutrient sensing, to incretin action, to the blunted secretion of putative insulin resistance hormone(s), to changes in the microbiota. Whatever the mechanism, metabolic surgery has the undoubted merit of exposing the central role of the small intestine in insulin sensitivity and glucose homeostasis.
Keywords: Bariatric surgery; Biliopancreatic bypass; Diabetes mellitus; Gastric bypass; Obesity; Sleeve gastrectomy.
Conflict of interest statement
V. Kamvissi-Lorenz, M. Raffaelli, and S. Bornstein declare that they have no conflict of interest. G. Mingrone declares personal fees from Novo Nordisk, Johnson and Johnson, and Fractyl, and grant support from Metacure. Human and Animal Rights All reported studies/experiments with human or animal subjects performed by the authors have been previously published and complied with all applicable ethical standards (including the Helsinki declaration and its amendments, institutional/national research committee standards, and international/national/institutional guidelines).
Figures
Similar articles
-
Intestinal peptide changes after bariatric and minimally invasive surgery: Relation to diabetes remission.Peptides. 2018 Feb;100:114-122. doi: 10.1016/j.peptides.2017.12.010. Peptides. 2018. PMID: 29412812 Review.
-
Neuro-modulation and bariatric surgery for type 2 diabetes mellitus.Int J Clin Pract Suppl. 2010 Feb;(166):53-8. doi: 10.1111/j.1742-1241.2009.02279.x. Int J Clin Pract Suppl. 2010. PMID: 20377665 Review.
-
Role of the incretin system in the remission of type 2 diabetes following bariatric surgery.Nutr Metab Cardiovasc Dis. 2008 Oct;18(8):574-9. doi: 10.1016/j.numecd.2008.07.004. Nutr Metab Cardiovasc Dis. 2008. PMID: 18790374
-
Incretins or anti-incretins? A new model for the "entero-pancreatic axis".Horm Metab Res. 2015 Jan;47(1):84-7. doi: 10.1055/s-0034-1394374. Epub 2014 Nov 11. Horm Metab Res. 2015. PMID: 25388925 Review.
-
Changes of insulin sensitivity and secretion after bariatric/metabolic surgery.Surg Obes Relat Dis. 2016 Jul;12(6):1199-205. doi: 10.1016/j.soard.2016.05.013. Epub 2016 May 13. Surg Obes Relat Dis. 2016. PMID: 27568471 Review.
Cited by
-
In-and-Out Molecular Changes Linked to the Type 2 Diabetes Remission after Bariatric Surgery: An Influence of Gut Microbes on Mitochondria Metabolism.Int J Mol Sci. 2018 Nov 24;19(12):3744. doi: 10.3390/ijms19123744. Int J Mol Sci. 2018. PMID: 30477251 Free PMC article.
-
A Meta-Analysis of the Efficacy of Prokinetic Agents against Glycemic Control.Gastroenterol Res Pract. 2019 Sep 9;2019:3014973. doi: 10.1155/2019/3014973. eCollection 2019. Gastroenterol Res Pract. 2019. PMID: 31582970 Free PMC article. Review.
-
Intestinal resection-associated metabolic syndrome.J Pediatr Surg. 2018 Jun;53(6):1142-1147. doi: 10.1016/j.jpedsurg.2018.02.077. Epub 2018 Mar 7. J Pediatr Surg. 2018. PMID: 29588076 Free PMC article.
-
Gut Microbiota Modifications and Weight Regain in Morbidly Obese Women After Roux-en-Y Gastric Bypass.Obes Surg. 2020 Dec;30(12):4958-4966. doi: 10.1007/s11695-020-04956-9. Epub 2020 Sep 11. Obes Surg. 2020. PMID: 32915360
-
A Gut-Centric Model of Metabolic Homeostasis.J Diabetes Sci Technol. 2022 Nov;16(6):1567-1574. doi: 10.1177/19322968211044523. Epub 2021 Oct 26. J Diabetes Sci Technol. 2022. PMID: 34697950 Free PMC article.
References
-
- Rubino F, Kaplan LM, Schauer PR, Cummings DE. The Diabetes Surgery Summit consensus conference: recommendations for the evaluation and use of gastrointestinal surgery to treat type 2 diabetes mellitus. Ann Surg. 251 Suppl 3:399–405. - PubMed
-
- Buchwald H, Varco RL. Metabolic surgery. New York: Grune and Stratton; 1978.
-
- Rubino F, Cummings DE. Surgery: the coming of age of metabolic surgery. Nat Rev Endocrinol. 8 Suppl 12:702–4. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
