

Increased Access to Professional Interpreters in the Hospital Improves Informed Consent for Patients with Limited English Proficiency
- PMID: 28185201
- PMCID: PMC5515780
- DOI: 10.1007/s11606-017-3983-4
Increased Access to Professional Interpreters in the Hospital Improves Informed Consent for Patients with Limited English Proficiency
Abstract
Background: Language barriers disrupt communication and impede informed consent for patients with limited English proficiency (LEP) undergoing healthcare procedures. Effective interventions for this disparity remain unclear.
Objective: Assess the impact of a bedside interpreter phone system intervention on informed consent for patients with LEP and compare outcomes to those of English speakers.
Design: Prospective, pre-post intervention implementation study using propensity analysis.
Subjects: Hospitalized patients undergoing invasive procedures on the cardiovascular, general surgery or orthopedic surgery floors.
Intervention: Installation of dual-handset interpreter phones at every bedside enabling 24-h immediate access to professional interpreters.
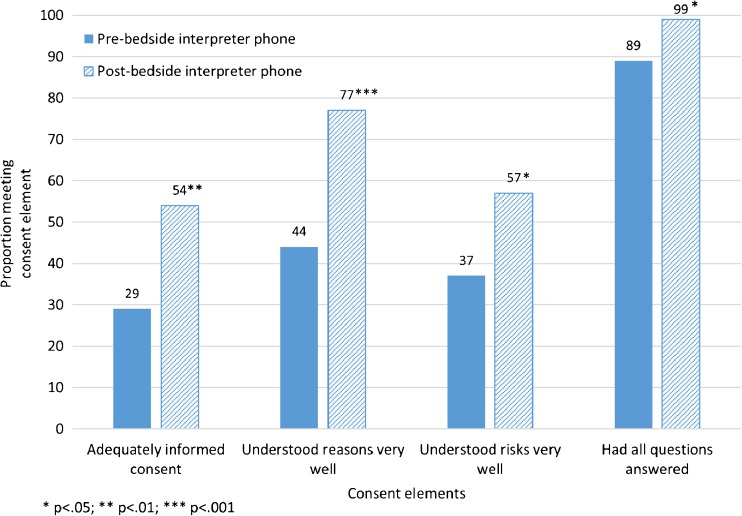
Main measures: Primary predictor: pre- vs. post-implementation group; secondary predictor: post-implementation patients with LEP vs. English speakers. Primary outcomes: three central informed consent elements, patient-reported understanding of the (1) reasons for and (2) risks of the procedure and (3) having had all questions answered. We considered consent adequately informed when all three elements were met.
Key results: We enrolled 152 Chinese- and Spanish-speaking patients with LEP (84 pre- and 68 post-implementation) and 86 English speakers. Post-implementation (vs. pre-implementation) patients with LEP were more likely to meet criteria for adequately informed consent (54% vs. 29%, p = 0.001) and, after propensity score adjustment, had significantly higher odds of adequately informed consent (AOR 2.56; 95% CI, 1.15-5.72) as well as of each consent element individually. However, compared to post-implementation English speakers, post-implementation patients with LEP had significantly lower adjusted odds of adequately informed consent (AOR, 0.38; 95% CI, 0.16-0.91).
Conclusions: A bedside interpreter phone system intervention to increase rapid access to professional interpreters was associated with improvements in patient-reported informed consent and should be considered by hospitals seeking to improve care for patients with LEP; however, these improvements did not eliminate the language-based disparity. Additional clinician educational interventions and more language-concordant care may be necessary for informed consent to equal that for English speakers.
Keywords: communication barriers; informed consent; language access; limited English proficiency; medical interpreters; physician-patient relations.
Conflict of interest statement
Compliance with Ethical Standards
The findings and conclusions in this article are those of the authors and do not necessarily represent the views or the official position(s) of the National Institutes of Health or any of the sponsoring organizations and agencies of the US government.
Conflicts of Interest
The authors report no conflicts of interest pertaining to this manuscript. An earlier version of this manuscript was presented at the Society of General Internal Medicine annual conference in San Diego, CA, in 2014.
Figures


Comment in
-
Language Barriers, Informed Consent, and Effective Caregiving.J Gen Intern Med. 2017 Aug;32(8):855-857. doi: 10.1007/s11606-017-4068-0. J Gen Intern Med. 2017. PMID: 28493178 Free PMC article. No abstract available.
-
Medicine, Politics, and the English Language.J Gen Intern Med. 2017 Aug;32(8):853-854. doi: 10.1007/s11606-017-4081-3. J Gen Intern Med. 2017. PMID: 28547722 Free PMC article. No abstract available.
References
-
- Berg JW, Appelbaum PS. Informed consent: legal theory and clinical practice. 2. Oxford: Oxford University Press; 2001.
-
- U.S. Census Bureau. American Community Survey, 2015 American Community Survey 1-Year Estimates; using American FactFinder. http://factfinder2.census.gov. Accessed December 15, 2016.
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
