

Tuberculous Peritonitis
- PMID: 28185616
- PMCID: PMC11687449
- DOI: 10.1128/microbiolspec.TNMI7-0006-2016
Tuberculous Peritonitis
Abstract
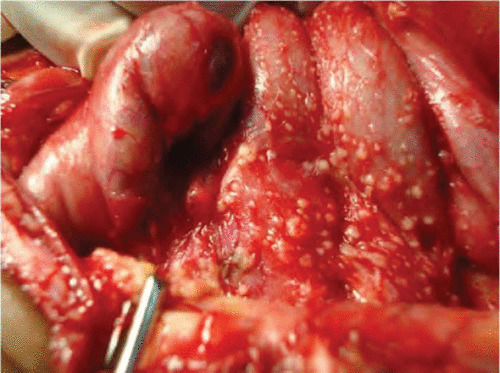
Tuberculous peritonitis is rare in the United States but continues to be reported to occur in certain high-risk populations, which include patients with AIDS or cirrhosis, patients on continuous ambulatory peritoneal dialysis, recent immigrants from areas of high endemicity, and those who are immunosuppressed. The diagnosis of this disease requires a high clinical index of suspicion and should be considered in the differential of ascites with a lymphocyte predominance and serum-ascitic albumin gradient of <1.1 mg/dl. Microbiological or pathological confirmation remains the gold standard for diagnosis. Ascitic fluid cultures have low yield, but peritoneoscopy with biopsy or cultures frequently confirms the diagnosis. Newer techniques with future application include determination of adenosine deaminase and interferon gamma levels in ascitic fluid. Ultrasound and computed tomography are frequently used to guide fluid aspiration and biopsies. Six months of treatment with antituberculosis therapy is adequate except in cases of drug-resistant tuberculosis. The role of steroids remains controversial. Surgical approaches may be required to deal with complications including bowel perforation, intestinal obstruction from adhesions, fistula formation, or bleeding.
Figures
References
-
- Borhanmanesh F, Hekmat K, Vaezzadeh K, Rezai HR. 1972. Tuberculous peritonitis. Prospective study of 32 cases in Iran. Ann Intern Med 76:567–572. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
