

Detailed Vascular Anatomy of the Human Retina by Projection-Resolved Optical Coherence Tomography Angiography
- PMID: 28186181
- PMCID: PMC5301488
- DOI: 10.1038/srep42201
Detailed Vascular Anatomy of the Human Retina by Projection-Resolved Optical Coherence Tomography Angiography
Abstract
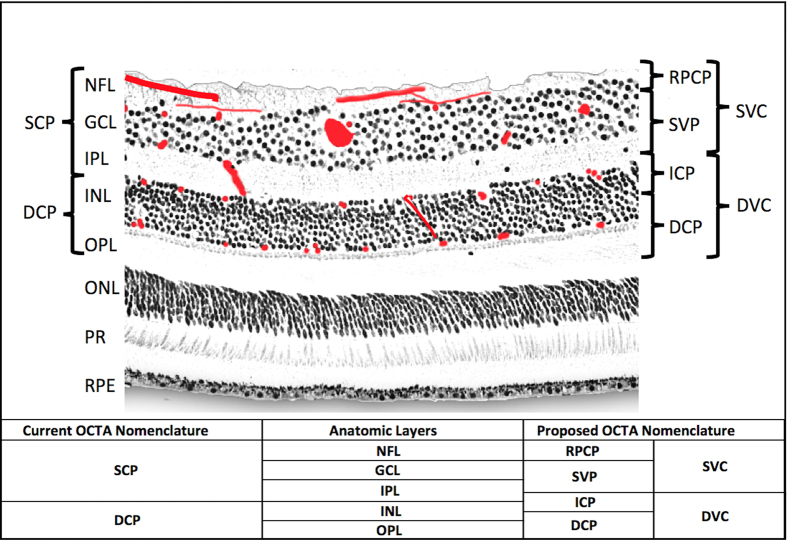
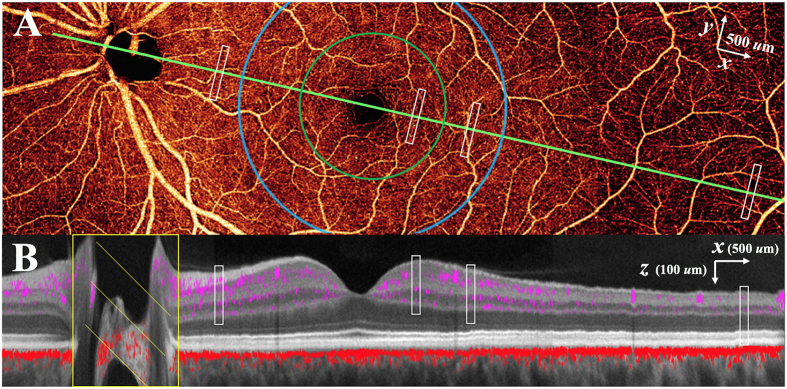
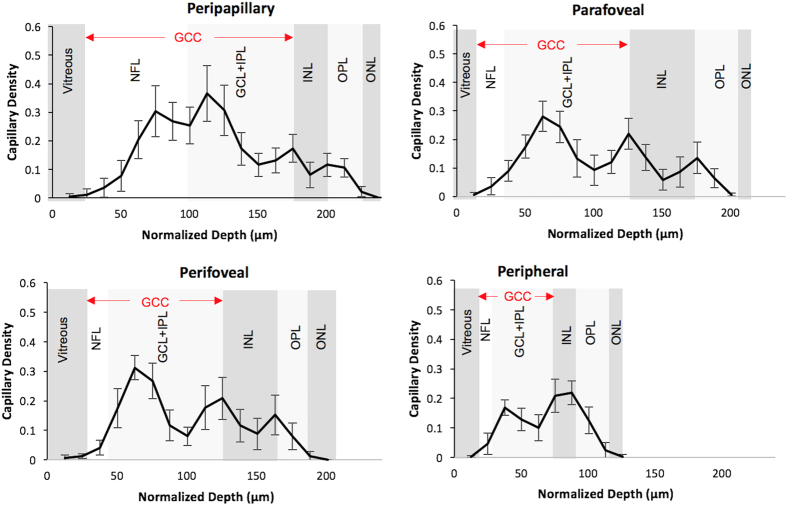
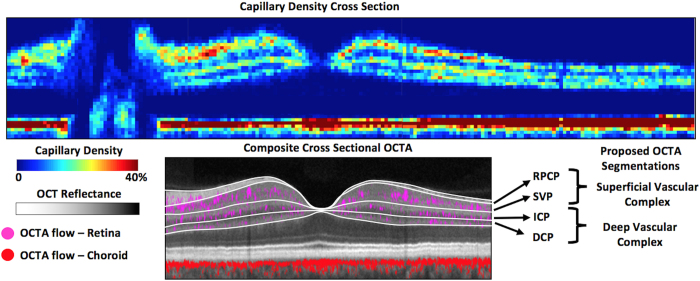
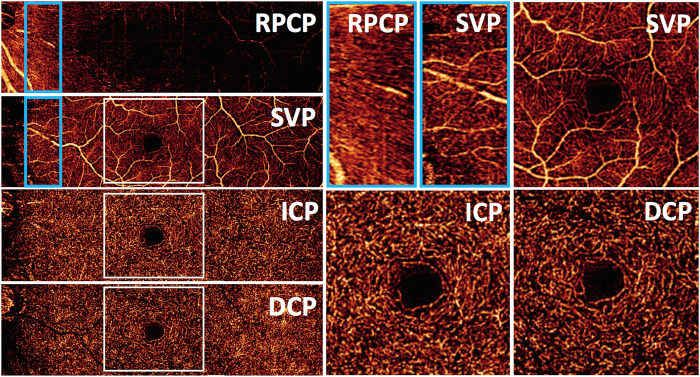
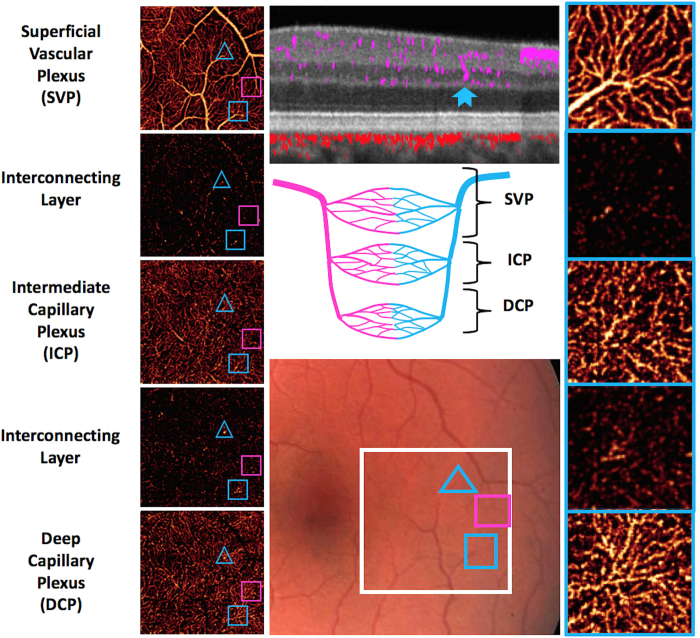
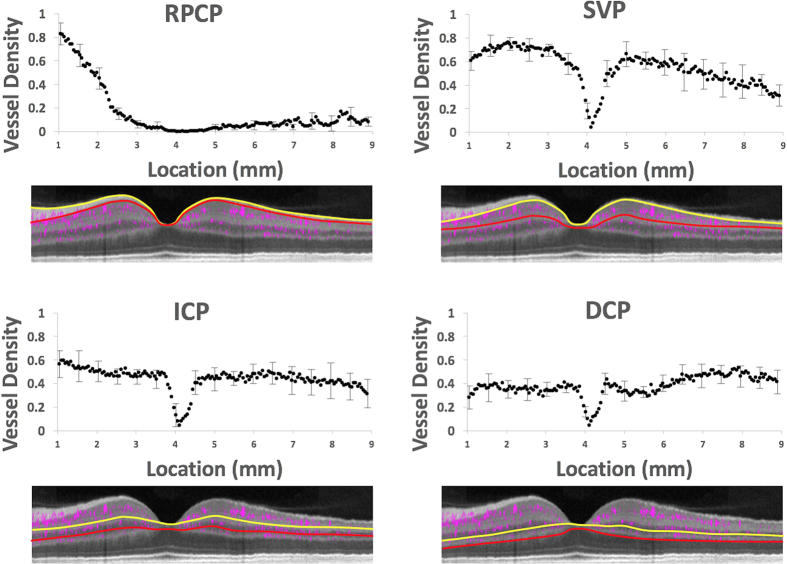
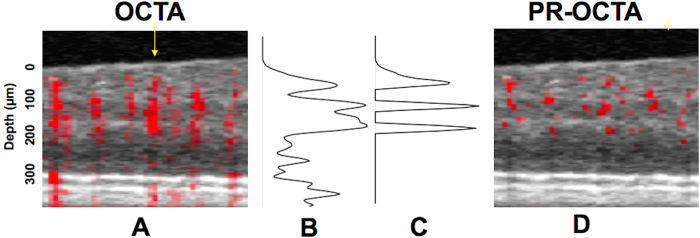
Optical coherence tomography angiography (OCTA) is a noninvasive method of 3D imaging of the retinal and choroidal circulations. However, vascular depth discrimination is limited by superficial vessels projecting flow signal artifact onto deeper layers. The projection-resolved (PR) OCTA algorithm improves depth resolution by removing projection artifact while retaining in-situ flow signal from real blood vessels in deeper layers. This novel technology allowed us to study the normal retinal vasculature in vivo with better depth resolution than previously possible. Our investigation in normal human volunteers revealed the presence of 2 to 4 distinct vascular plexuses in the retina, depending on location relative to the optic disc and fovea. The vascular pattern in these retinal plexuses and interconnecting layers are consistent with previous histologic studies. Based on these data, we propose an improved system of nomenclature and segmentation boundaries for detailed 3-dimensional retinal vascular anatomy by OCTA. This could serve as a basis for future investigation of both normal retinal anatomy, as well as vascular malformations, nonperfusion, and neovascularization.
Conflict of interest statement
Oregon Health & Science University (OHSU), Yali Jia, and David Huang have a significant financial interest in Optovue, Inc., a company that may have a commercial interest in the results of this research and technology. These potential conflicts of interest have been reviewed and managed by OHSU. David Huang receives patent royalties from Carl Zeiss Meditec, Inc. Other authors do not have financial interest in the subject of this article.
Figures
References
-
- Provis J. M. Development of the primate retinal vasculature. Progress in Retinal and Eye Research 20, 799–821 (2001). - PubMed
-
- Stone J., van Driel D., Valter K., Rees S. & Provis J. The locations of mitochondria in mammalian photoreceptors: relation to retinal vasculature. Brain Res. 1189, 58–69 (2008). - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
