

Inhibition of Receptor-Interacting Protein Kinase 1 with Necrostatin-1s ameliorates disease progression in elastase-induced mouse abdominal aortic aneurysm model
- PMID: 28186202
- PMCID: PMC5301478
- DOI: 10.1038/srep42159
Inhibition of Receptor-Interacting Protein Kinase 1 with Necrostatin-1s ameliorates disease progression in elastase-induced mouse abdominal aortic aneurysm model
Abstract
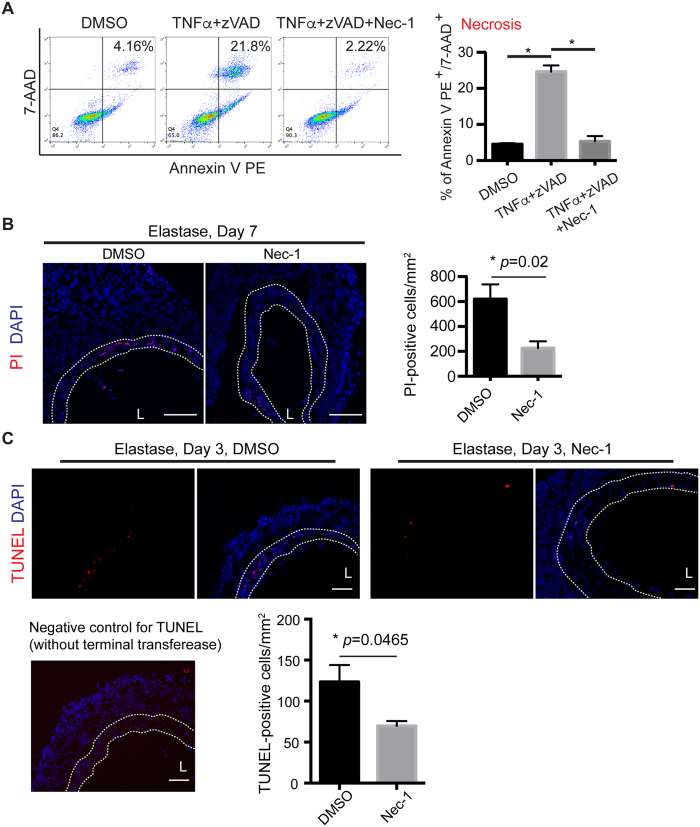
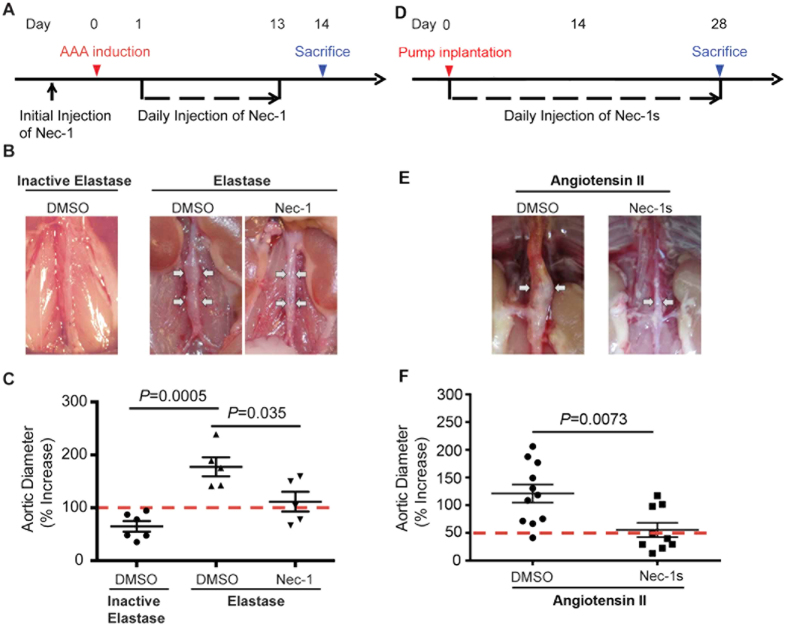
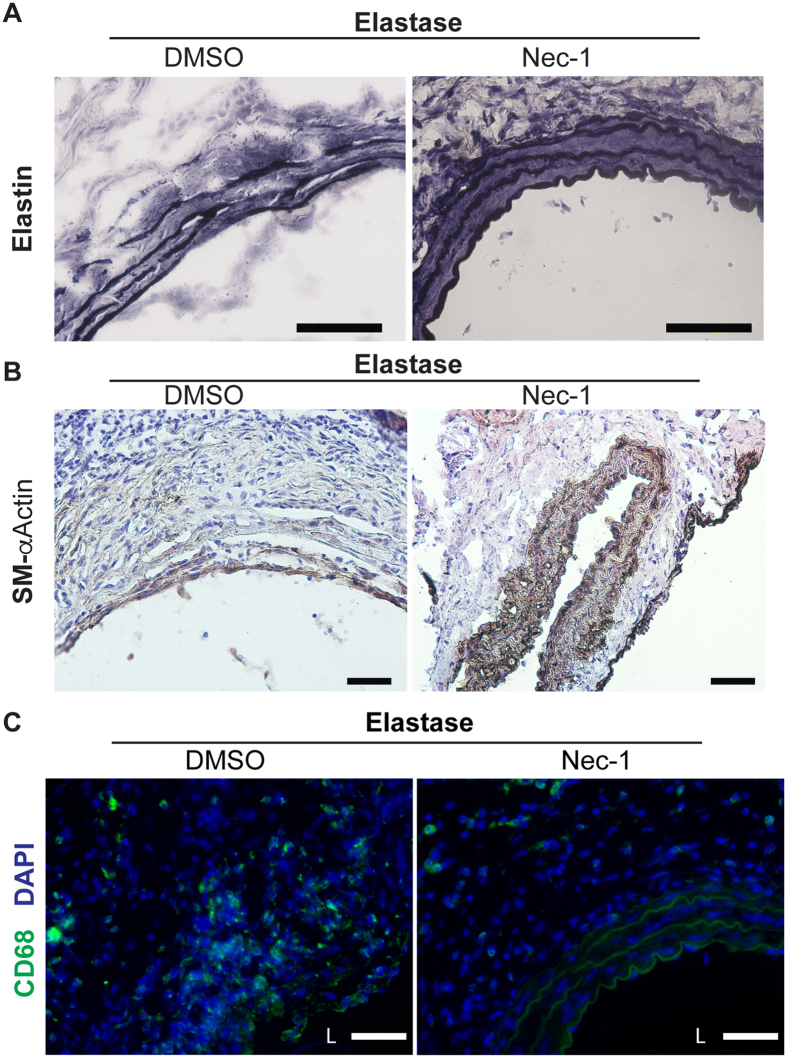
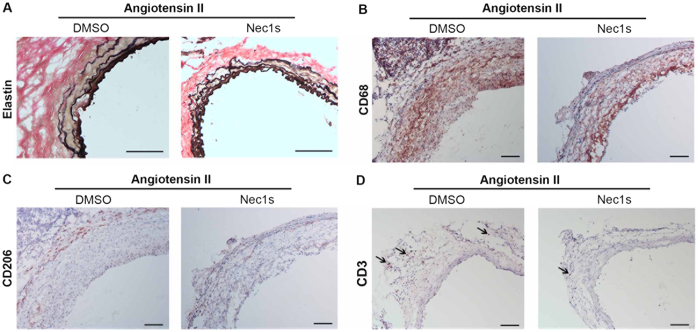
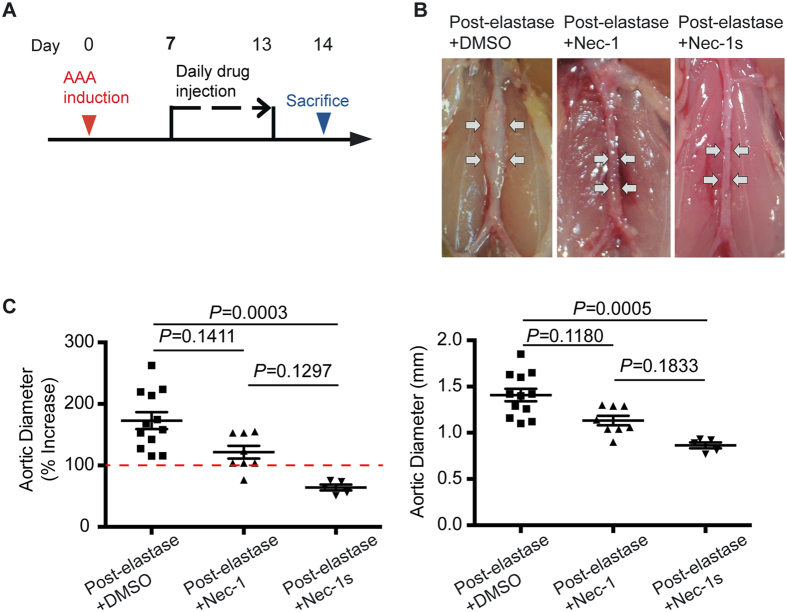
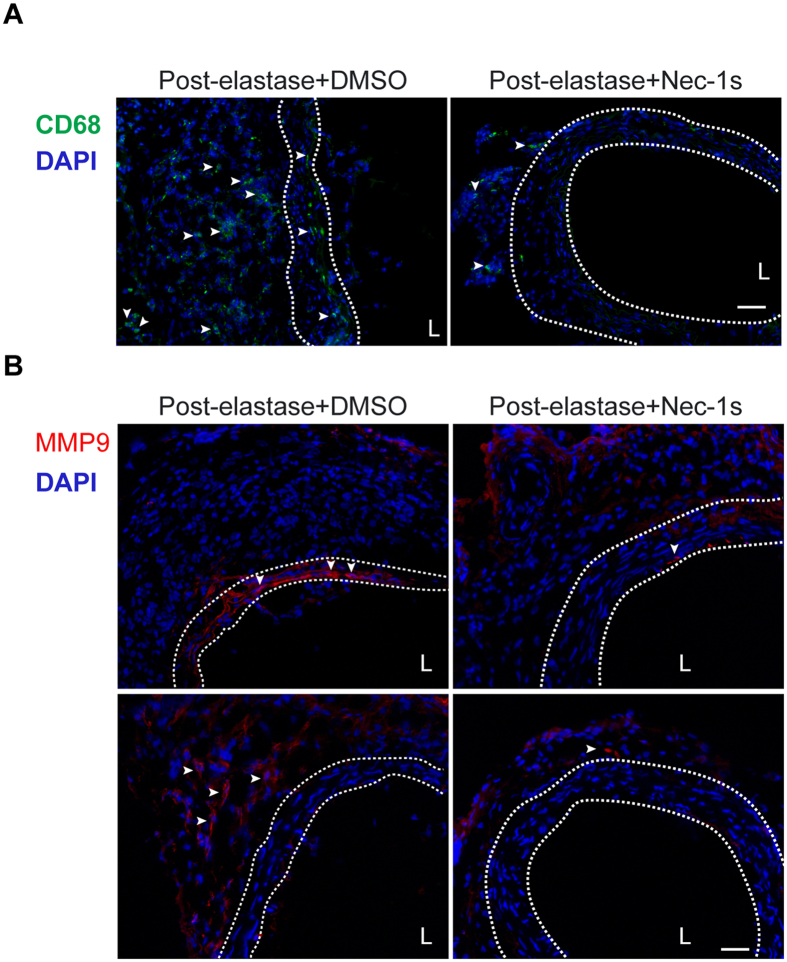
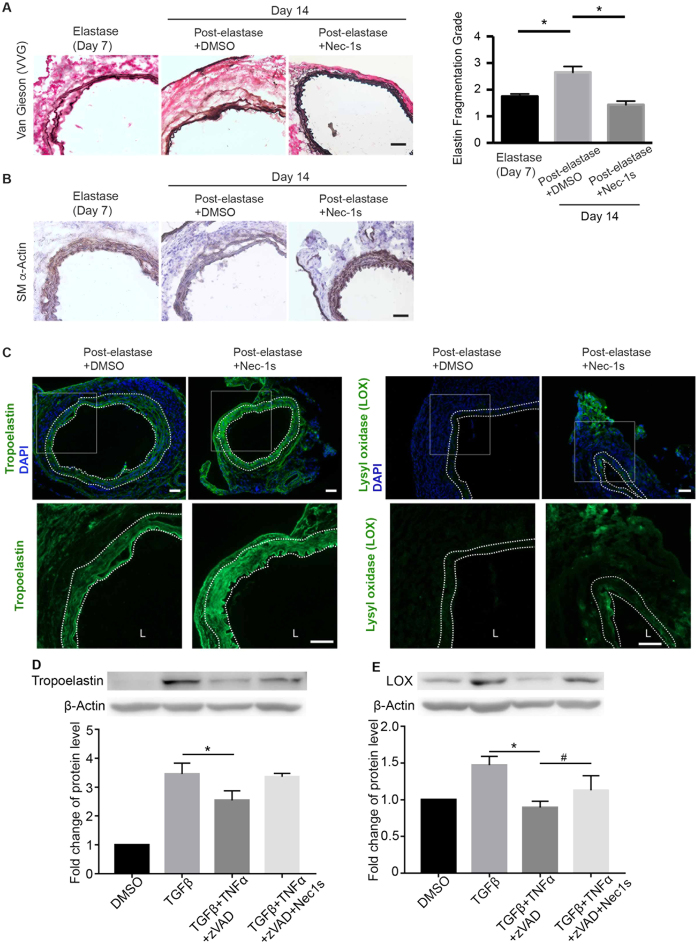
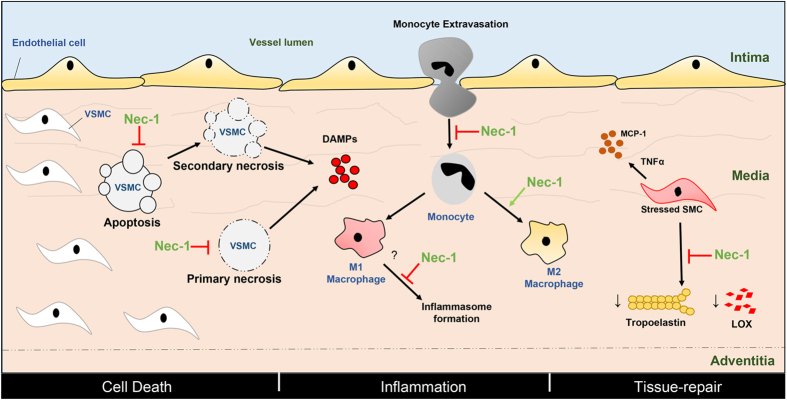
Abdominal aortic aneurysm (AAA) is a common aortic disease with a progressive nature. There is no approved pharmacological treatment to effectively slow aneurysm growth or prevent rupture. Necroptosis is a form of programmed necrosis that is regulated by receptor-interacting protein kinases (RIPs). We have recently demonstrated that the lack of RIP3 in mice prevented aneurysm formation. The goal of the current study is to test whether perturbing necroptosis affects progression of existing aneurysm using the RIP1 inhibitors Necrostatin-1 (Nec-1) and an optimized form of Nec-1, 7-Cl-O-Nec-1 (Nec-1s). Seven days after aneurysm induction by elastase perfusion, mice were randomly administered DMSO, Nec-1 (3.2 mg/kg/day) and Nec-1s (1.6 mg/kg/day) via intraperitoneal injection. Upon sacrifice on day 14 postaneurysm induction, the aortic expansion in the Nec-1s group (64.12 ± 4.80%) was significantly smaller than that of the DMSO group (172.80 ± 13.68%) (P < 0.05). The mean aortic diameter of Nec-1 treated mice appeared to be smaller (121.60 ± 10.40%) than the DMSO group, though the difference was not statistically significant (P = 0.1). Histologically, the aortic structure of Nec-1s-treated mice appeared normal, with continuous and organized elastin laminae and abundant αActin-expressing SMCs. Moreover, Nect-1s treatment diminished macrophage infiltration and MMP9 accumulation and increased aortic levels of tropoelastin and lysyl oxidase. Together, our data suggest that pharmacological inhibition of necroptosis with Nec-1s stabilizes pre-existing aneurysms by diminishing inflammation and promoting connective tissue repair.
Conflict of interest statement
The authors declare no competing financial interests.
Figures
References
-
- Powell J. T. & Greenhalgh R. M. Clinical practice. Small abdominal aortic aneurysms. The New England journal of medicine 348, 1895–1901 (2003). - PubMed
-
- Kent K. C. Clinical practice. Abdominal aortic aneurysms. The New England journal of medicine 371, 2101–2108 (2014). - PubMed
-
- Lederle F. A. et al.. Prevalence and associations of abdominal aortic aneurysm detected through screening. Aneurysm Detection and Management (ADAM) Veterans Affairs Cooperative Study Group. Annals of internal medicine 126, 441–449 (1997). - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Miscellaneous
