

Cerebral blood flow, frontal lobe oxygenation and intra-arterial blood pressure during sprint exercise in normoxia and severe acute hypoxia in humans
- PMID: 28186430
- PMCID: PMC5757439
- DOI: 10.1177/0271678X17691986
Cerebral blood flow, frontal lobe oxygenation and intra-arterial blood pressure during sprint exercise in normoxia and severe acute hypoxia in humans
Abstract
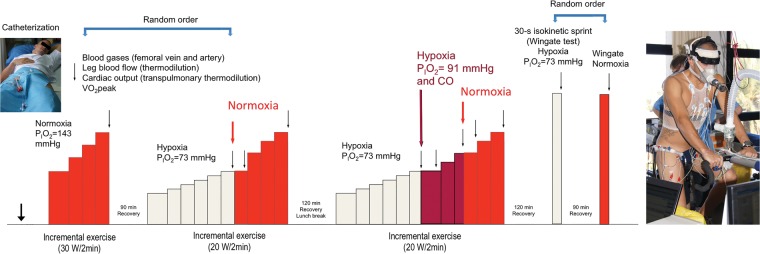
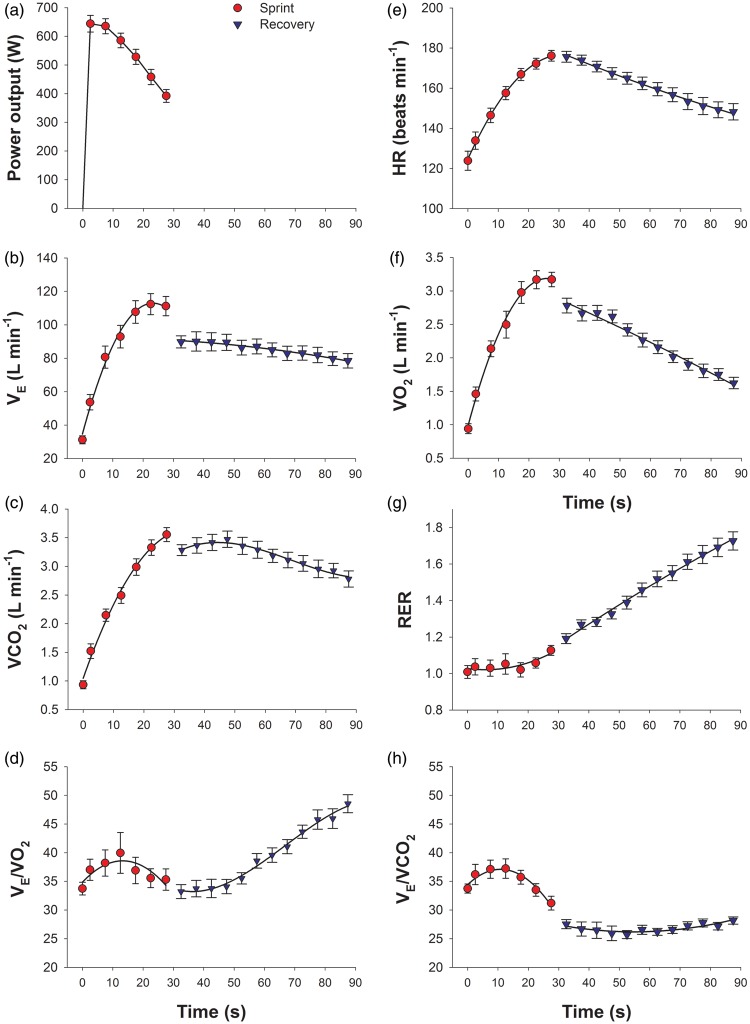
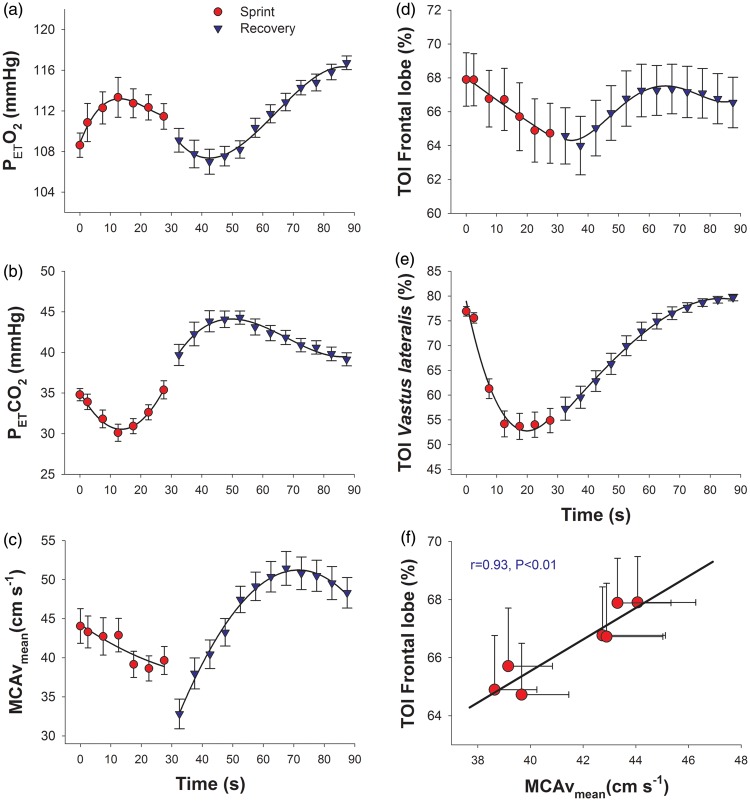
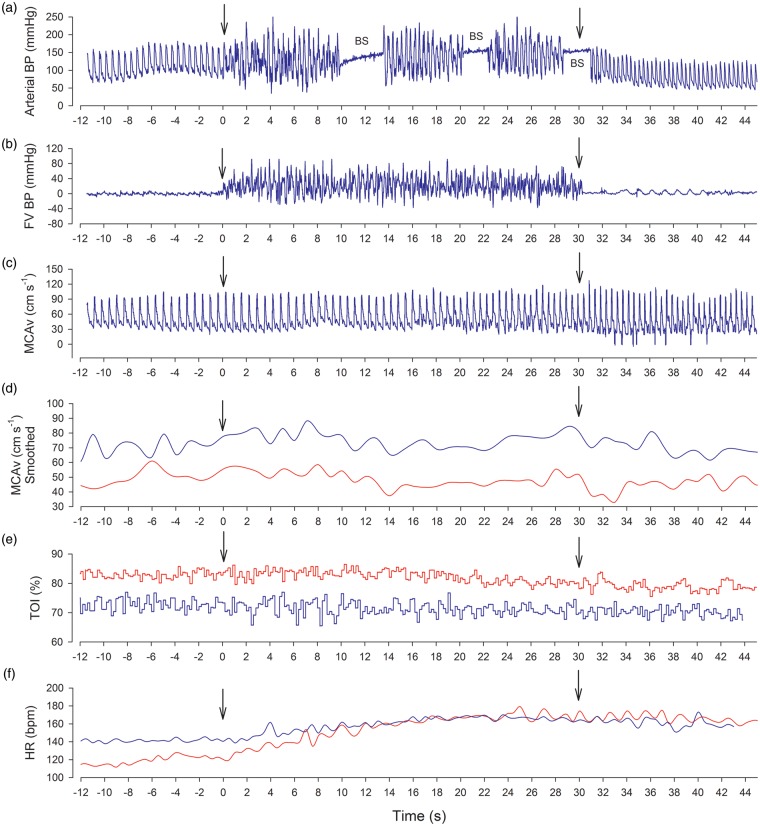
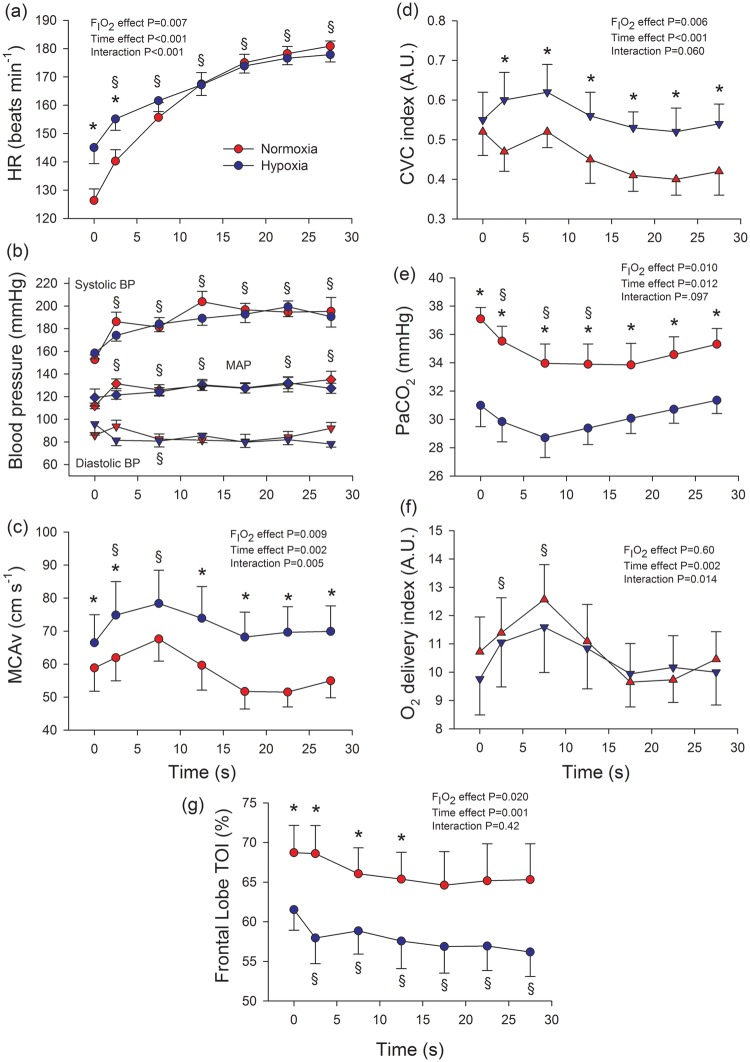
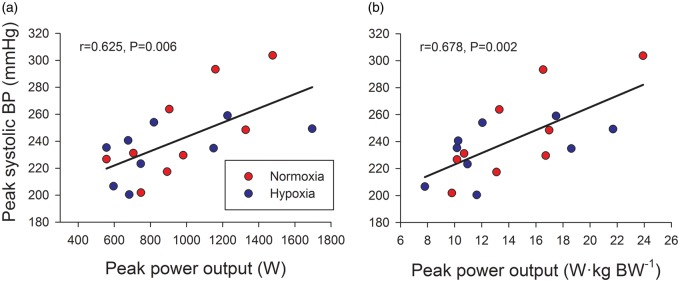
Cerebral blood flow (CBF) is regulated to secure brain O2 delivery while simultaneously avoiding hyperperfusion; however, both requisites may conflict during sprint exercise. To determine whether brain O2 delivery or CBF is prioritized, young men performed sprint exercise in normoxia and hypoxia (PIO2 = 73 mmHg). During the sprints, cardiac output increased to ∼22 L min-1, mean arterial pressure to ∼131 mmHg and peak systolic blood pressure ranged between 200 and 304 mmHg. Middle-cerebral artery velocity (MCAv) increased to peak values (∼16%) after 7.5 s and decreased to pre-exercise values towards the end of the sprint. When the sprints in normoxia were preceded by a reduced PETCO2, CBF and frontal lobe oxygenation decreased in parallel ( r = 0.93, P < 0.01). In hypoxia, MCAv was increased by 25%, due to a 26% greater vascular conductance, despite 4-6 mmHg lower PaCO2 in hypoxia than normoxia. This vasodilation fully accounted for the 22 % lower CaO2 in hypoxia, leading to a similar brain O2 delivery during the sprints regardless of PIO2. In conclusion, when a conflict exists between preserving brain O2 delivery or restraining CBF to avoid potential damage by an elevated perfusion pressure, the priority is given to brain O2 delivery.
Keywords: Exercise; cerebral blood flow; cerebral haemodynamics; high altitude; hypertension.
Figures
References
-
- Lassen NA. Cerebral blood flow and oxygen consumption in man. Physiol Rev 1959; 39: 183–238. - PubMed
-
- Calbet JA, Gonzalez-Alonso J, Helge JW, et al. Central and peripheral hemodynamics in exercising humans: leg vs arm exercise. Scand J Med Sci Sports 2015; 25(Suppl 4): 144–157. - PubMed
-
- MacDougall JD, Tuxen D, Sale DG, et al. Arterial blood pressure response to heavy resistance exercise. J Appl Physiol 1985; 58: 785–790. - PubMed
-
- van Mook WN, Rennenberg RJ, Schurink GW, et al. Cerebral hyperperfusion syndrome. Lancet Neurol 2005; 4: 877–888. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
