

Population pharmacokinetics and pharmacodynamics of linezolid-induced thrombocytopenia in hospitalized patients
- PMID: 28186644
- PMCID: PMC5510085
- DOI: 10.1111/bcp.13262
Population pharmacokinetics and pharmacodynamics of linezolid-induced thrombocytopenia in hospitalized patients
Abstract
Aims: Thrombocytopenia is among the most important adverse effects of linezolid treatment. Linezolid-induced thrombocytopenia incidence varies considerably but has been associated with impaired renal function. We investigated the pharmacodynamic mechanism (myelosuppression or enhanced platelet destruction) and the role of impaired renal function (RF) in the development of thrombocytopenia.
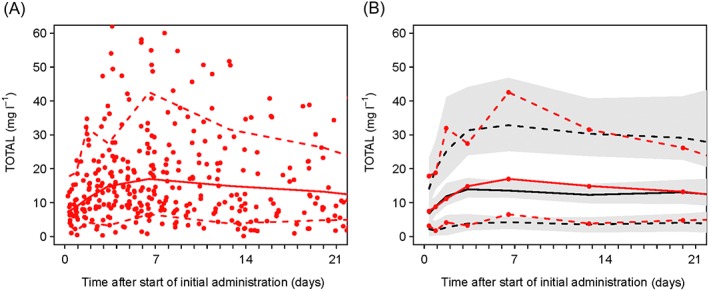
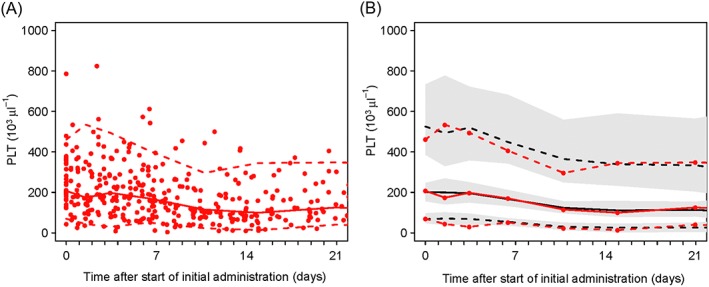
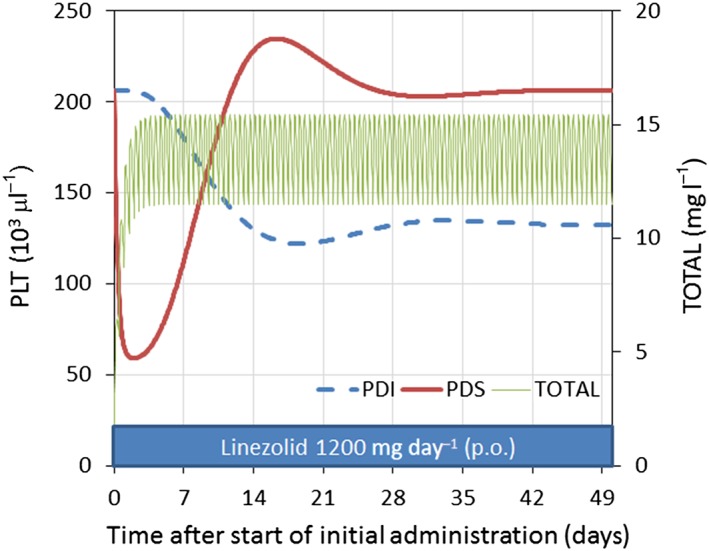
Methods: The pharmacokinetics of linezolid were described with a two-compartment distribution model with first-order absorption and elimination. RF was calculated using the expected creatinine clearance. The decrease platelets by linezolid exposure was assumed to occur by one of two mechanisms: inhibition of the formation of platelets (PDI) or stimulation of the elimination (PDS) of platelets.
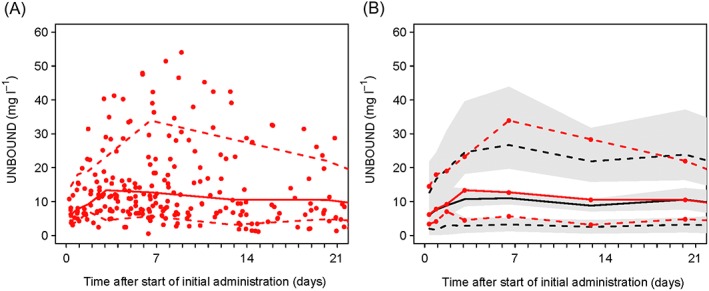
Results: About 50% of elimination was found to be explained by renal clearance (normal RF). The population mean estimated plasma protein binding of linezolid was 18% [95% confidence interval (CI) 16%, 20%] and was independent of the observed concentrations. The estimated mixture model fraction of patients with a platelet count decreased due to PDI was 0.97 (95% CI 0.87, 1.00), so the fraction due to PDS was 0.03. RF had no influence on linezolid pharmacodynamics.
Conclusion: We have described the influence of weight, renal function, age and plasma protein binding on the pharmacokinetics of linezolid. This combined pharmacokinetic, pharmacodynamic and turnover model identified that the most common mechanism of thrombocytopenia associated with linezolid is PDI. Impaired RF increases thrombocytopenia by a pharmacokinetic mechanism. The linezolid dose should be reduced in RF.
Keywords: linezolid; methicillin-resistant Staphylococcus aureus; mixture model; pharmacometrics; thrombocytopenia; turnover model.
© 2017 The British Pharmacological Society.
Figures

References
-
- Dryden MS. Linezolid pharmacokinetics and pharmacodynamics in clinical treatment. J Antimicrob Chemother 2011; 66 (Suppl. 4)): iv7–iv15. - PubMed
-
- Lovering AM, Zhang J, Bannister GC, Lankester BJA, Brown JHM, Narendra G, et al. Penetration of linezolid into bone, fat, muscle and haematoma of patients undergoing routine hip replacement. J Antimicrob Chemother 2002; 50: 73–77. - PubMed
-
- Tsuji Y, Hashimoto W, Taniguchi S, Hiraki Y, Mizoguchi A, Yukawa E, et al. Pharmacokinetics of linezolid in the mediastinum and pleural space. Int J Infect Dis 2013; 17: E1060–E1061. - PubMed
-
- Tsuji Y, Hiraki Y, Matsumoto K, Mizoguchi A, Sadoh S, Kobayashi T, et al. Pharmacokinetics and protein binding of linezolid in cerebrospinal fluid and serum in a case of post‐neurosurgical bacterial meningitis. Scand J Infect Dis 2011; 43: 982–985. - PubMed
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
