

Impact of scheduled appointments on cervical screening participation in Norway: a randomised intervention
- PMID: 28186949
- PMCID: PMC5128903
- DOI: 10.1136/bmjopen-2016-013728
Impact of scheduled appointments on cervical screening participation in Norway: a randomised intervention
Abstract
Background: The main barrier to optimal effect in many established population-based screening programmes against cervical cancer is low participation. In Norway, a routine health service integrated population-based screening programme has been running since 1995, using open invitations and reminders. The aim of this randomised health service study was to pilot scheduled appointments and assess their potential for increased participation.
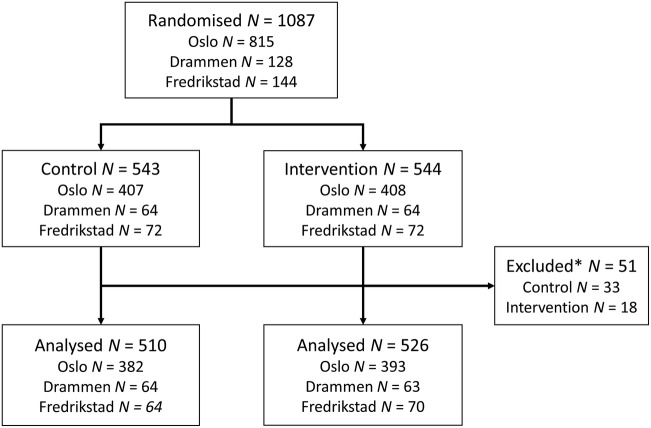
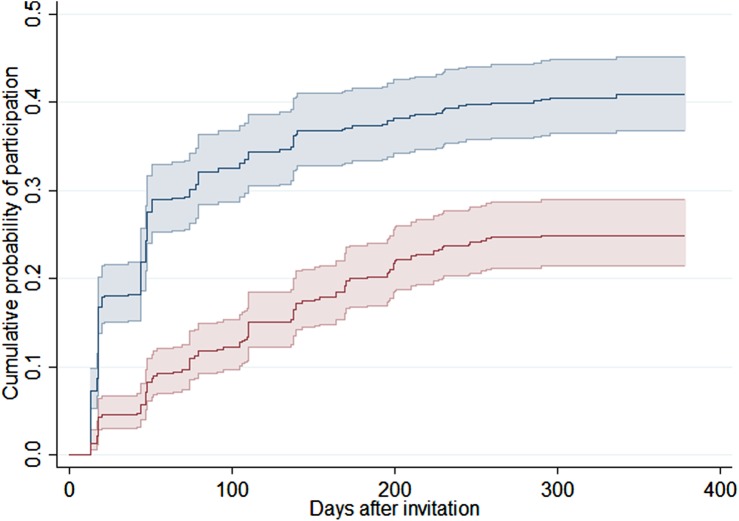
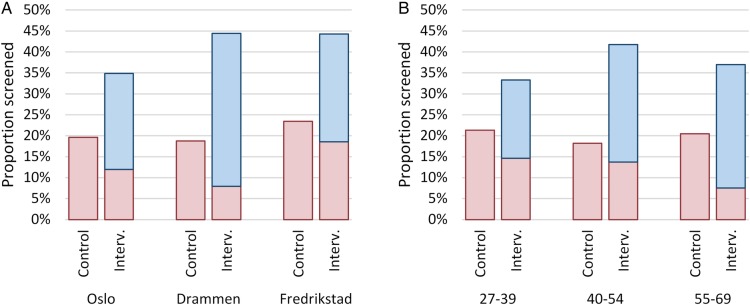
Methods: Within the national screening programme, we randomised 1087 women overdue for screening to receive invitations with scheduled appointments (intervention) or the standard open reminders (control). Letters were sent 2-4 weeks before the scheduled appointments at three centres: a midwife clinic, a public healthcare centre and a general practitioner centre. The primary outcome was participation at 6 months of follow-up. Secondary outcomes were participation at 1 and 3 months. Risk ratios (RRs) overall, and stratified by screening centre, age group and previous participation, were calculated using log-binomial regression.
Results: At 6 months, 20% of the 510 women in the control group and 37% of the 526 women in the intervention group had participated in screening, excluding 51 women in total from analysis due to participation just before invitation and therefore not yet visible in the central records. The RR for participation at 6 months was 1.9 (95% CI 1.5 to 2.3). There was no significant heterogeneity between centres or age groups. Participation increased among women both with (RR 1.7; 95% CI 1.4 to 2.1) and without (RR 3.5; 95% CI 1.3 to 9.2) previous participation. The RRs for participation at 1 and 3 months were 4.0 (95% CI 2.6 to 6.2) and 2.7 (95% CI 2.1 to 3.5), respectively.
Conclusions: Scheduled appointments increased screening participation consistently across all target ages and screening centres among women overdue for screening. Participation increased also among women with no previous records of cervical screening.
Keywords: PREVENTIVE MEDICINE.
Published by the BMJ Publishing Group Limited. For permission to use (where not already granted under a licence) please go to http://www.bmj.com/company/products-services/rights-and-licensing/.
Conflict of interest statement
Conflicts of Interest: None declared.
Figures
References
-
- Skare GB, Lönnberg S. Masseundersøkelsen mot livmorhalskreft. Årsrapport 2013–2014. [Cervical screening programme annual report 2013–2014] Oslo: Cancer Registry of Norway, 2015.
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical