

Primary, Adaptive, and Acquired Resistance to Cancer Immunotherapy
- PMID: 28187290
- PMCID: PMC5391692
- DOI: 10.1016/j.cell.2017.01.017
Primary, Adaptive, and Acquired Resistance to Cancer Immunotherapy
Abstract
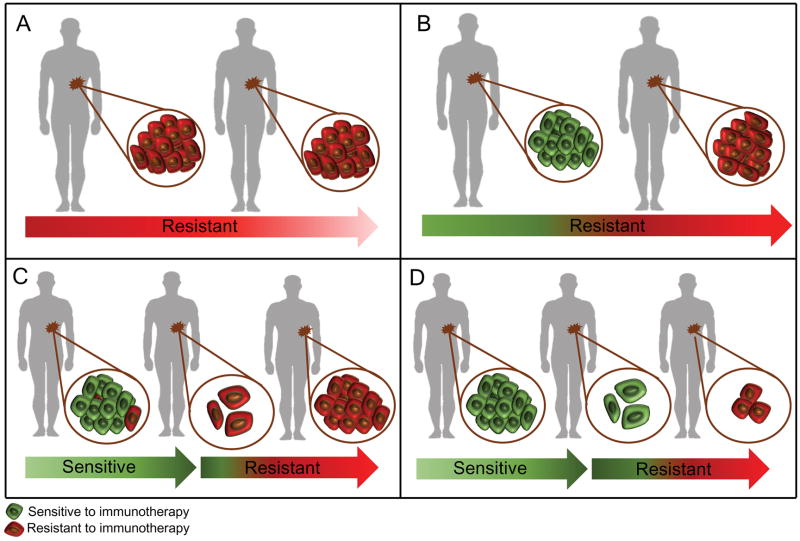
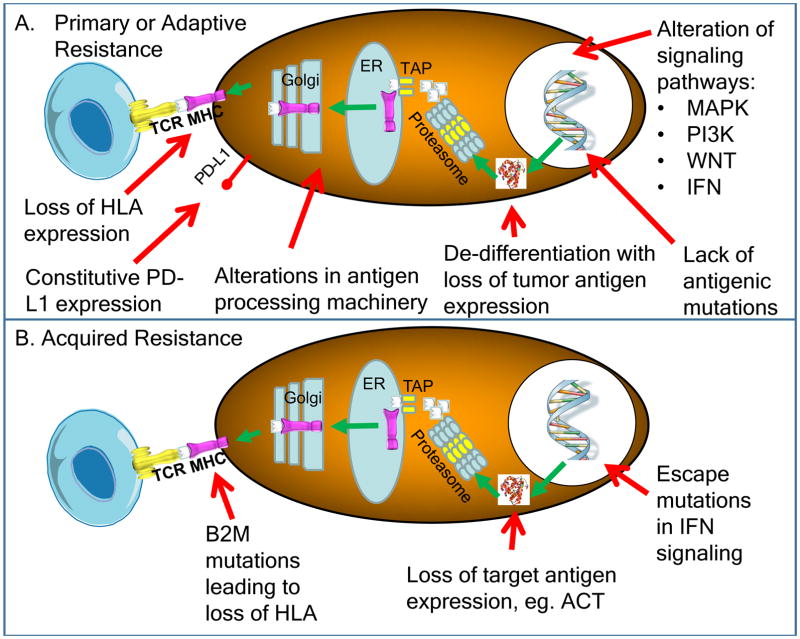
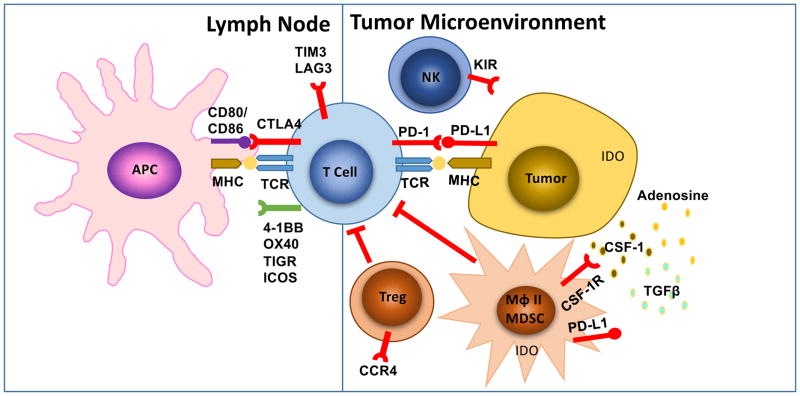
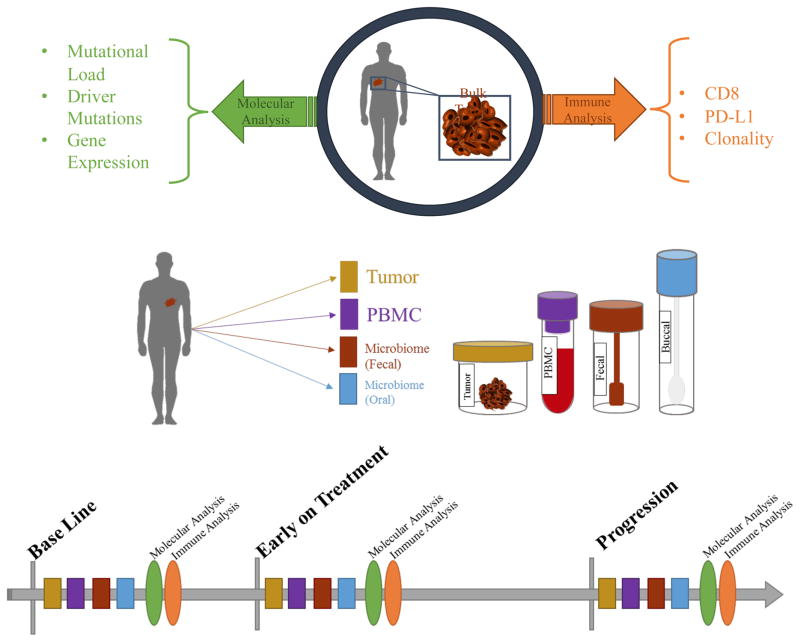
Cancer immunotherapy can induce long lasting responses in patients with metastatic cancers of a wide range of histologies. Broadening the clinical applicability of these treatments requires an improved understanding of the mechanisms limiting cancer immunotherapy. The interactions between the immune system and cancer cells are continuous, dynamic, and evolving from the initial establishment of a cancer cell to the development of metastatic disease, which is dependent on immune evasion. As the molecular mechanisms of resistance to immunotherapy are elucidated, actionable strategies to prevent or treat them may be derived to improve clinical outcomes for patients.
Keywords: T cells; immunotherapy; resistance mechanisms.
Copyright © 2017 Elsevier Inc. All rights reserved.
Figures
References
-
- Allard B, Turcotte M, Spring K, Pommey S, Royal I, Stagg J. Anti-CD73 therapy impairs tumor angiogenesis. International Journal of Cancer. 2014;134:1466–1473. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
