

Variations in the cost of formal and informal health care for patients with advanced chronic disease and refractory breathlessness: A cross-sectional secondary analysis
- PMID: 28190370
- PMCID: PMC5405827
- DOI: 10.1177/0269216317690994
Variations in the cost of formal and informal health care for patients with advanced chronic disease and refractory breathlessness: A cross-sectional secondary analysis
Abstract
Background: Refractory breathlessness in advanced chronic disease leads to high levels of disability, anxiety and social isolation. These result in high health-resource use, although this is not quantified.
Aims: To measure the cost of care for patients with advanced disease and refractory breathlessness and to identify factors associated with high costs.
Design: A cross-sectional secondary analysis of data from a randomised controlled trial.
Setting/participants: Patients with advanced chronic disease and refractory breathlessness recruited from three National Health Service hospitals and via general practitioners in South London.
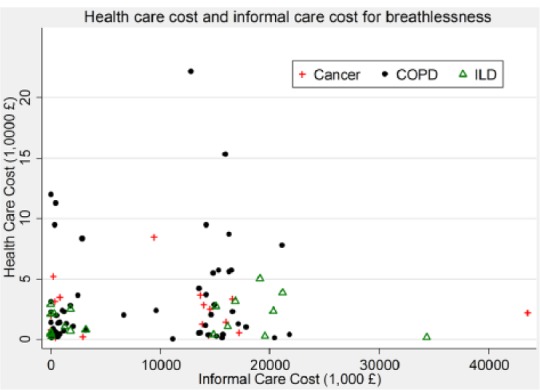
Results: Of 105 patients recruited, the mean cost of formal care was £3253 (standard deviation £3652) for 3 months. The largest contributions to formal-care cost were hospital admissions (>60%), and palliative care contributed <1%. When informal care was included, the total cost increased by >250% to £11,507 (standard deviation £9911). Increased patient disability resulting from breathlessness was associated with high cost (£629 per unit increase in disability score; p = 0.006). Increased breathlessness on exertion and the presence of an informal carer were also significantly associated with high cost. Patients with chronic obstructive pulmonary disease tended to have higher healthcare costs than other patients.
Conclusion: Informal carers contribute significantly to the care of patients with advanced disease and refractory breathlessness. Disability resulting from breathlessness is an important clinical cost driver. It is important for policy makers to support and acknowledge the contributions of informal carers. Further research is required to assess the clinical- and cost-effectiveness of palliative care interventions in reducing disability resulting from breathlessness in this patient group.
Keywords: Healthcare costs; breathlessness; cancer; chronic disease; chronic obstructive pulmonary disease; dyspnoea; end-of-life care; heart failure; interstitial lung diseases; palliative care; terminal care.
Conflict of interest statement
Figures

References
-
- Currow DC, Abernethy AP, Ko DN. The active identification and management of chronic refractory breathlessness is a human right. Thorax 2014; 69: 393–394. - PubMed
-
- Higginson IJ, Bausewein C, Reilly CC, et al. An integrated palliative and respiratory care service for patients with advanced disease and refractory breathlessness: a randomised controlled trial. Lancet Respir Med 2014; 2: 979–987. - PubMed
-
- Sorenson HM. Palliative care for lung disease: start early, stay late. Lancet Respir Med 2013; 1: 279–280. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
