

High-density Lipoprotein and Low-density Lipoprotein Therapeutic Approaches in Acute Coronary Syndromes
- PMID: 28190386
- PMCID: PMC5633711
- DOI: 10.2174/1573403X13666170209145622
High-density Lipoprotein and Low-density Lipoprotein Therapeutic Approaches in Acute Coronary Syndromes
Abstract
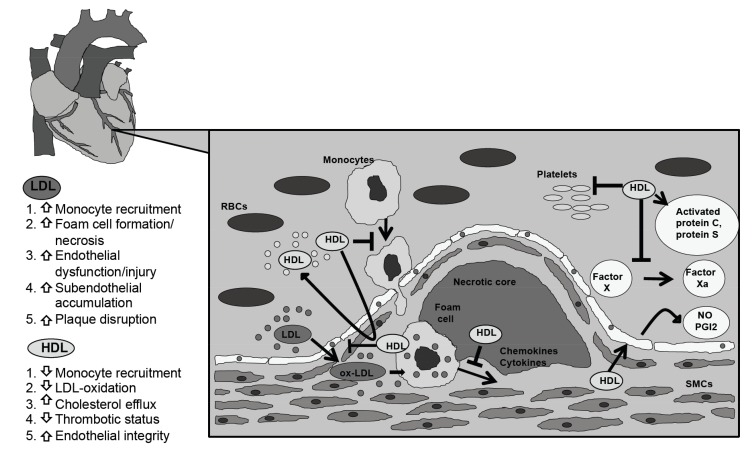
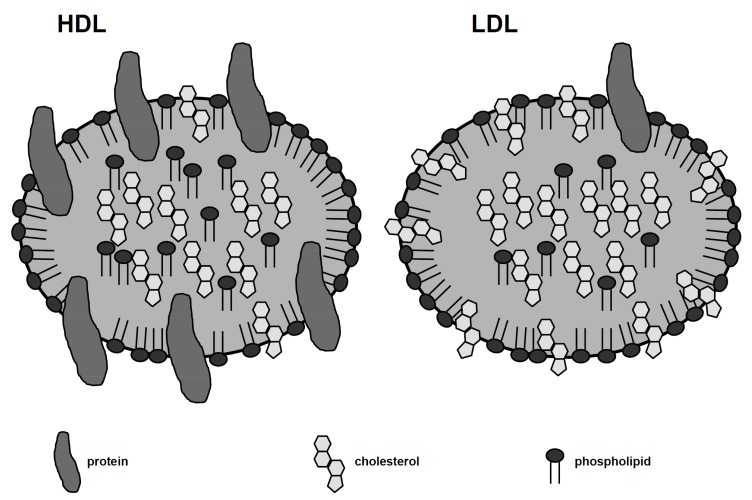
Background: Low-density lipoprotein cholesterol (LDL), and especially its oxidized form, renders the atherosclerotic plaque vulnerable to rupture in acute coronary syndromes (ACS). On the other hand, high-density lipoprotein (HDL) is considered an anti-atherogenic molecule. The more recent HDL-targeted drugs may prove to be superior to those used before. Indeed, delipidated HDL and HDL mimetics are efficient in increasing HDL levels, while the apoA-I upregulation with RVX-208 appears to offer a clinical benefit which is beyond the HDL related effects. HDL treatment however has not shown a significant improvement in the outcomes of patients with ACS so far, studies have therefore focused again on LDL. In addition to statins and ezetimibe, novel drugs such as PSCK9 inhibitors and apolipoprotein B inhibitors appear to be both effective and safe for patients with hyperlipidemia.
Conclusion: Data suggest these could potentially improve the cardiovascular outcomes of patient with ACS. Yet, there is still research to be done, in order to confirm whether ACS patients would benefit from LDL- or HDL-targeted therapies or a combination of both.
Keywords: High-density lipoprotein; acute coronary syndromes; atherosclerosis; ezetimibe; lipidlowering drugs; low-density lipoprotein; outcomes; statins.
Copyright© Bentham Science Publishers; For any queries, please email at epub@benthamscience.org.
Figures
References
-
- Prevention of cardiovascular events and death with pravastatin in patients with coronary heart disease and a broad range of initial cholesterol levels. The Long-Term Intervention with Pravastatin in Ischaemic Disease (LIPID) Study Group. N. Engl. J. Med. 1998;339(19):1349–1357. - PubMed
-
- Correia L.C., Rocha M.S., Esteves J.P. HDL-cholesterol level provides additional prognosis in acute coronary syndromes. Int. J. Cardiol. 2009;136(3):307–314. - PubMed
-
- Gordon T., Castelli W.P., Hjortland M.C., Kannel W.B., Dawber T.R. High density lipoprotein as a protective factor against coronary heart disease. The Framingham Study. Am. J. Med. 1977;62(5):707–714. - PubMed
-
- Sacks F.M., Pfeffer M.A., Moye L.A., et al. The effect of pravastatin on coronary events after myocardial infarction in patients with average cholesterol levels. Cholesterol and Recurrent Events Trial investigators. N. Engl. J. Med. 1996;335(14):1001–1009. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
