

Abortion health services in Canada: Results of a 2012 national survey
- PMID: 28192276
- PMCID: PMC4830677
Abortion health services in Canada: Results of a 2012 national survey
Abstract
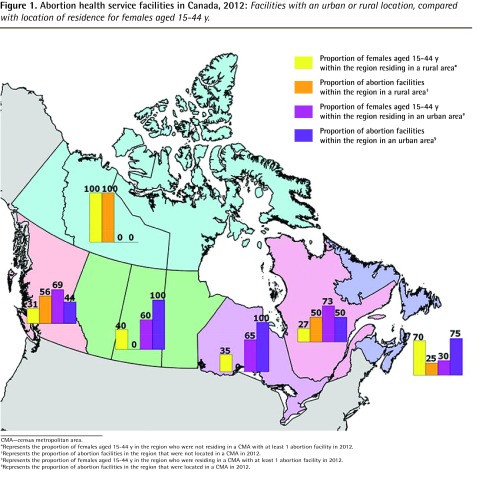
Objective: To determine the location of Canadian abortion services relative to where reproductive-age women reside, and the characteristics of abortion facilities and providers.
Design: An international survey was adapted for Canadian relevance. Public sources and professional networks were used to identify facilities. The bilingual survey was distributed by mail and e-mail from July to November 2013.
Setting: Canada.
Participants: A total of 94 abortion facilities were identified.
Main outcome measures: The number and location of services were compared with the distribution of reproductive-age women by location of residence.
Results: We identified 94 Canadian facilities providing abortion in 2012, with 48.9% in Quebec. The response rate was 83.0% (78 of 94). Facilities in every jurisdiction with services responded. In Quebec and British Columbia abortion services are nearly equally present in large urban centres and rural locations throughout the provinces; in other Canadian provinces services are chiefly located in large urban areas. No abortion services were identified in Prince Edward Island. Respondents reported provision of 75 650 abortions in 2012 (including 4.0% by medical abortion). Canadian facilities reported minimal or no harassment, in stark contrast to American facilities that responded to the same survey.
Conclusion: Access to abortion services varies by region across Canada. Services are not equitably distributed in relation to the regions where reproductive-age women reside. British Columbia and Quebec have demonstrated effective strategies to address disparities. Health policy and service improvements have the potential to address current abortion access inequity in Canada. These measures include improved access to mifepristone for medical abortion; provincial policies to support abortion services; routine abortion training within family medicine residency programs; and increasing the scope of practice for nurses and midwives to include abortion provision.
Objectif: Vérifier où sont situés les services canadiens d’avortement par rapport aux endroits où habitent les femmes en âge d’enfanter et déterminer les caractéristiques des établissements et des médecins qui offrent des avortements.
Type d’étude: On a adapté une enquête internationale pour tenir compte du contexte canadien. On s’est servi de données publiques et de réseaux professionnels pour identifier les établissements. Le questionnaire a été distribué dans les deux langues par voie postale et par courriel, de juillet à novembre 2013.
Contexte: Le Canada.
Participants: Un total de 94 cliniques d’avortement.
Principaux paramètres à l’étude: Le nombre et les lieux des services d’avortement ont été comparés à la répartition des femmes en âge de procréer, selon le lieu de résidence.
Résultats: On a répertorié 94 établissements canadiens qui offraient des avortements en 2012, dont 48,9 % au Québec. Le taux de réponse était de 83,0 % (78 sur 94). On a reçu des réponses de chacune des régions administratives où ces services existaient. Au Québec et en Colombie-Britannique, les services d’avortement sont répartis à peu près également entre les grands centres urbains et les régions rurales; dans les autres provinces canadiennes, les services sont principalement dans les grands centres urbains. Aucun service de cette nature n’a été trouvé à l’Île-du-Prince-Édouard. Les répondants on dit avoir fait 75 650 avortements en 2012, dont 4,0 % d’avortements médicaux. Les établissements consultés sont rarement victimes de menaces ou de violence, ce qui contraste fortement avec les établissements américains qui avaient répondu à la même enquête.
Conclusion: Au Canada, l’accès aux services d’avortement varie beaucoup selon les régions. La distribution régionale de ces services ne tient pas compte des endroits où résident des femmes en âge de procréer. Le Québec et la Colombie-Britannique ont adopté des stratégies efficaces pour tenir compte de ces disparités. Avec des politiques appropriées et de meilleurs services, on pourrait éventuellement corriger ces inégalités au Canada. Les mesures pourraient comprendre un meilleur accès au mifépristone pour l’avortement médical; des politiques provinciales pour appuyer les services d’avortement; l’inclusion obligatoire de programmes de formation sur l’avortement durant la résidence en médecine familiale; et un élargissement du champ de pratique des infirmières et des sages-femmes pour leur permettre de faire des avortements.
Copyright© the College of Family Physicians of Canada.
Figures
References
-
- Norman WV. Induced abortion in Canada 1974–2005: trends over the first generation with legal access. Contraception. 2012;85(2):185–91. Epub 2011 Aug 4. - PubMed
-
- Canada Health Act. R.S.C. 1985 c C-6. Available from: http://laws-lois.justice.gc.ca/eng/acts/c-6/fulltext.html. Accessed 2015 Feb 28.
-
- Leeson H. Constitutional jurisdiction over health and health care services in Canada. In: McIntosh T, Forest PG, Marchildon GP, editors. The governance of health care in Canada. The Romanow papers. Vol. 3. Toronto, ON: University of Toronto Press; 2004. pp. 50–82.
-
- Sethna C, Doull M. Spatial disparities and travel to freestanding abortion clinics in Canada. Womens Stud Int Forum. 2013;38:52–62.
-
- Kaposy C. Improving abortion access in Canada. Health Care Anal. 2010;18(1):17–34. Epub 2008 Sep 27. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical