

Does dystonic muscle activity affect sense of effort in cervical dystonia?
- PMID: 28192488
- PMCID: PMC5305099
- DOI: 10.1371/journal.pone.0172019
Does dystonic muscle activity affect sense of effort in cervical dystonia?
Abstract
Background: Focal dystonia has been associated with deficient processing of sense of effort cues. However, corresponding studies are lacking in cervical dystonia (CD). We hypothesized that dystonic muscle activity would perturb neck force control based on sense of effort cues.
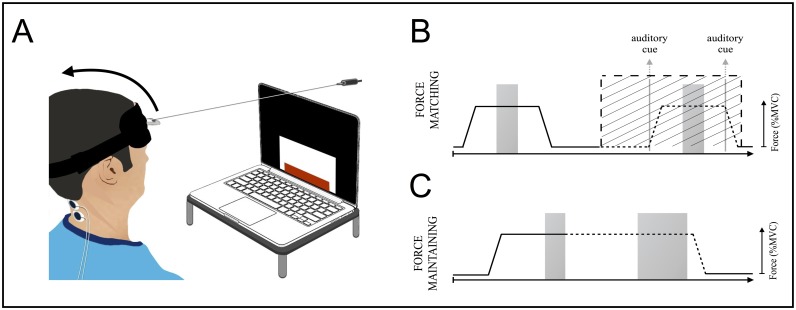
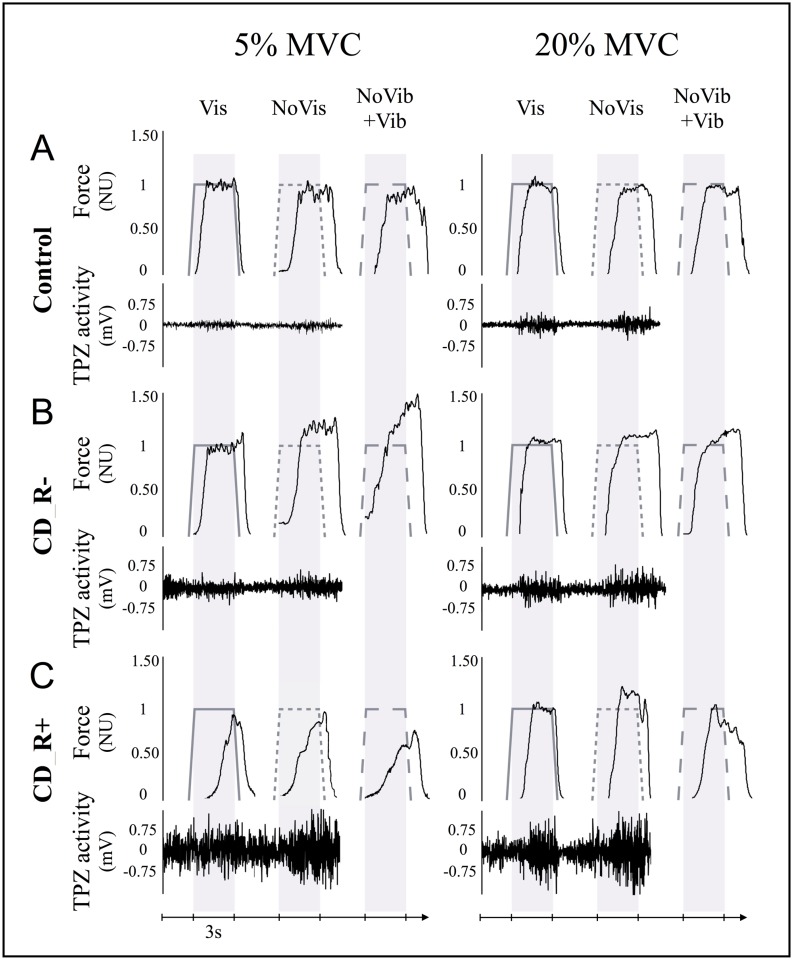
Methods: Neck extension force control was investigated in 18 CD patients with different clinical features (7 with and 11 without retrocollis) and in 19 control subjects. Subjects performed force-matching and force-maintaining tasks at 5% and 20% of maximum voluntary contraction (MVC). Three task conditions were tested: i) with visual force feedback, ii) without visual feedback (requiring use of sense of effort), iii) without visual feedback, but with neck extensor muscle vibration (modifying muscle afferent cues). Trapezius muscle activity was recorded using electromyography (EMG).
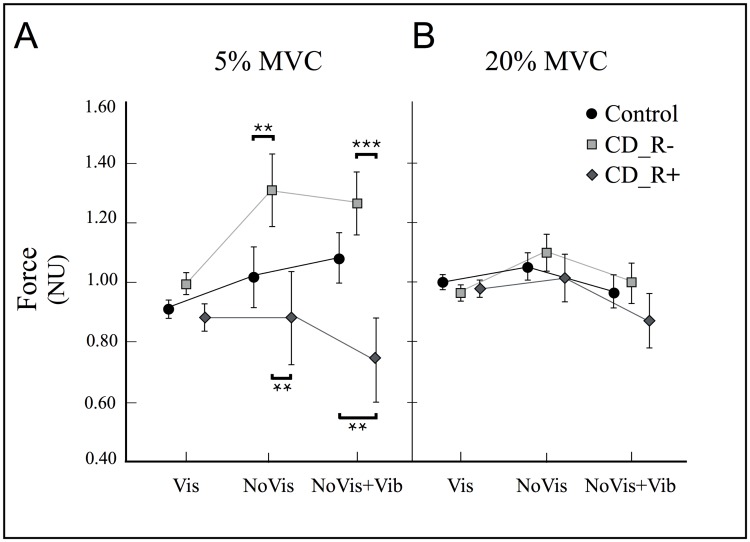
Results: CD patients did not differ in task performance from healthy subjects when using visual feedback (ANOVA, p>0.7). In contrast, when relying on sense of effort cues (without visual feedback, 5% MVC), force control was impaired in patients without retrocollis (p = 0.006), but not in patients with retrocollis (p>0.2). Compared to controls, muscle vibration without visual feedback significantly affected performance in patients with retrocollis (p<0.001), but not in patients without retrocollis. Extensor EMG during rest, included as covariate in ANOVA, explained these group differences.
Conclusion: This study shows that muscle afferent feedback biases sense of effort cues when controlling neck forces in patients with CD. The bias acts on peripheral or central sense of effort cues depending on whether the task involves dystonic muscles. This may explain why patients with retrocollis more accurately matched isometric neck extension forces. This highlights the need to consider clinical features (pattern of dystonic muscles) when evaluating sensorimotor integration in CD.
Conflict of interest statement
LC reports grants from Université Pierre et Marie Curie, Paris VI, outside the submitted work. SS reports personal fees from Allergan, personal fees from Ipsen, personal fees from Merz-Pharma, outside the submitted work. VG has nothing to disclose. SM reports grants from Fondation Paul Bennetot, outside the submitted work. MV reports grants from INSERM, grants from APHP, grants from APTES, grants from France Parkinson, grants from AMADYS, personal fees from Movement Disorders Society, outside the submitted work; and Member of the advisory board for Merz and Medtronic. PGL reports grants from Gloria and Jacques Gosweiler Foundation, outside the submitted work and owns shares in Aggero MedTech AB, a company commercializing a measurement instrument for spasticity. In addition, PGL and MAM have patented a method for measurement of manual dexterity (EP2659835A1). JPB reports personal fees from MERZ-PHARMA, personal fees from IPSEN, grants from AMADYS, grants from AFREK, outside the submitted work. This does not alter the authors’ adherence to PLOS ONE policies on sharing data and materials.
Figures
Similar articles
-
Improved identification of dystonic cervical muscles via abnormal muscle activity during isometric contractions.J Neurol Sci. 2015 Jul 15;354(1-2):10-6. doi: 10.1016/j.jns.2015.03.047. Epub 2015 Apr 9. J Neurol Sci. 2015. PMID: 25972112
-
Dystonic neck muscles show a shift in relative autospectral power during isometric contractions.Clin Neurophysiol. 2017 Oct;128(10):1937-1945. doi: 10.1016/j.clinph.2017.06.258. Epub 2017 Jul 17. Clin Neurophysiol. 2017. PMID: 28826024
-
The effect of changes in head posture on the patterns of muscle activity in cervical dystonia (CD).Mov Disord. 1998 May;13(3):490-6. doi: 10.1002/mds.870130320. Mov Disord. 1998. PMID: 9613743
-
Cervical dystonia pathophysiology and treatment options.Drugs. 2001;61(13):1921-43. doi: 10.2165/00003495-200161130-00004. Drugs. 2001. PMID: 11708764 Review.
-
Neurorehabilitation in dystonia: a holistic perspective.J Neural Transm (Vienna). 2021 Apr;128(4):549-558. doi: 10.1007/s00702-020-02265-0. Epub 2020 Oct 24. J Neural Transm (Vienna). 2021. PMID: 33099684 Free PMC article. Review.
Cited by
-
Combination of anodal tDCS of the cerebellum with a goal-oriented motor training to treat cervical dystonia: a pilot case series.Front Neurol. 2024 Apr 30;15:1381390. doi: 10.3389/fneur.2024.1381390. eCollection 2024. Front Neurol. 2024. PMID: 38746658 Free PMC article.
-
The Influence of External Forces on Wrist Proprioception.Front Hum Neurosci. 2017 Aug 31;11:440. doi: 10.3389/fnhum.2017.00440. eCollection 2017. Front Hum Neurosci. 2017. PMID: 28912703 Free PMC article.
References
-
- Boccagni C, Carpaneto J, Micera S, Bagnato S, Galardi G. Motion analysis in cervical dystonia. Neurol Sci. 2008. December;29(6):375–81. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
