

The Down syndrome brain in the presence and absence of fibrillar β-amyloidosis
- PMID: 28192686
- PMCID: PMC5391869
- DOI: 10.1016/j.neurobiolaging.2017.01.009
The Down syndrome brain in the presence and absence of fibrillar β-amyloidosis
Abstract
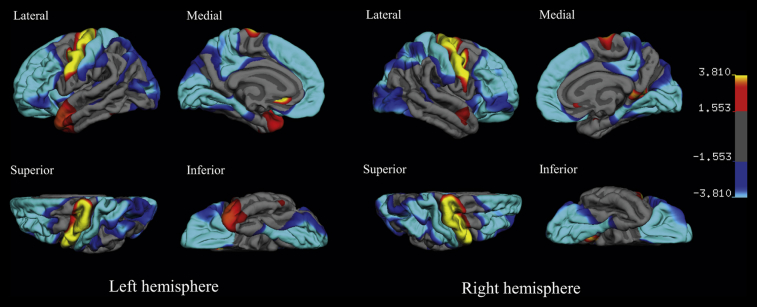
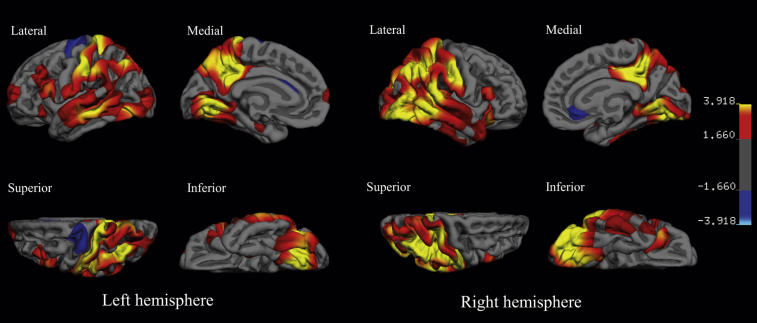
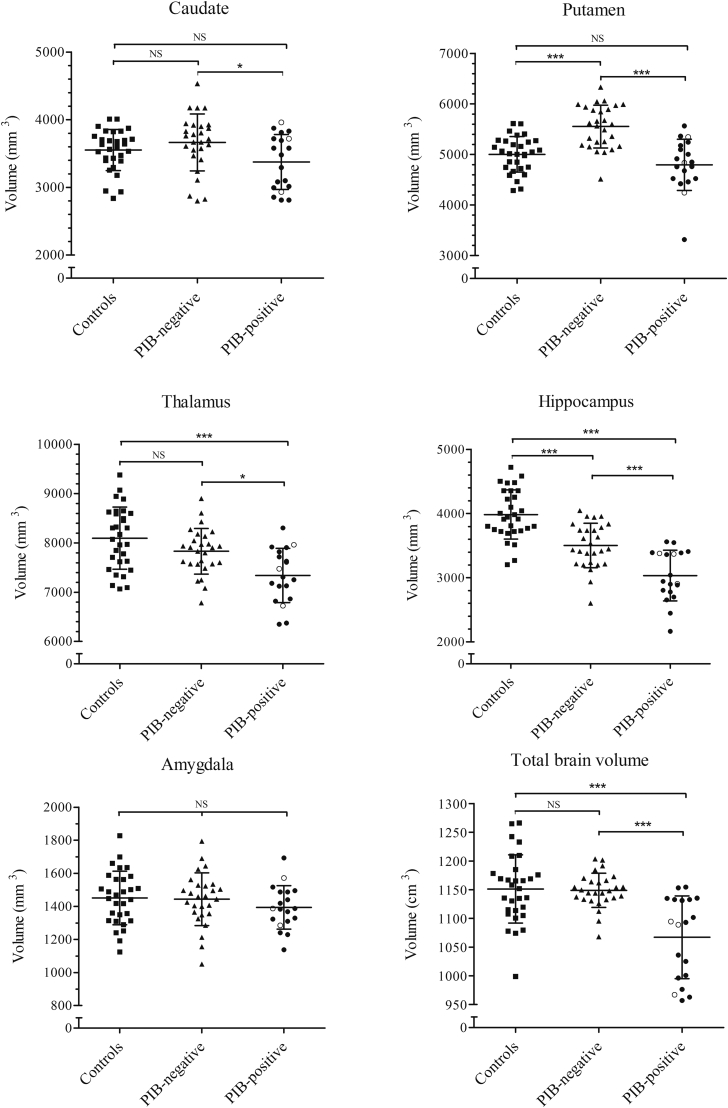
People with Down syndrome (DS) have a neurodevelopmentally distinct brain and invariably developed amyloid neuropathology by age 50. This cross-sectional study aimed to provide a detailed account of DS brain morphology and the changes occuring with amyloid neuropathology. Forty-six adults with DS underwent structural and amyloid imaging-the latter using Pittsburgh compound B (PIB) to stratify the cohort into PIB-positive (n = 19) and PIB-negative (n = 27). Age-matched controls (n = 30) underwent structural imaging. Group differences in deep gray matter volumetry and cortical thickness were studied. PIB-negative people with DS have neurodevelopmentally atypical brain, characterized by disproportionately thicker frontal and occipitoparietal cortex and thinner motor cortex and temporal pole with larger putamina and smaller hippocampi than controls. In the presence of amyloid neuropathology, the DS brains demonstrated a strikingly similar pattern of posterior dominant cortical thinning and subcortical atrophy in the hippocampus, thalamus, and striatum, to that observed in non-DS Alzheimer's disease. Care must be taken to avoid underestimating amyloid-associated morphologic changes in DS due to disproportionate size of some subcortical structures and thickness of the cortex.
Keywords: Alzheimer's disease; Amyloid; Cortical thickness; Down syndrome; Gray matter volume.
Copyright © 2017 The Authors. Published by Elsevier Inc. All rights reserved.
Figures
References
-
- Aizenstein H.J., Nebes R.D., Saxton J.A., Price J.C., Mathis C.A., Tsopelas N.D., Ziolko S.K., James J.A., Snitz B.E., Houck P.R., Bi W., Cohen A.D., Lopresti B.J., DeKosky S.T., Halligan E.M., Klunk W.E. Frequent amyloid deposition without significant cognitive impairment among the elderly. Arch. Neurol. 2008;65:1509–1517. - PMC - PubMed
-
- Annus T., Wilson L.R., Hong Y.T., Acosta–Cabronero J., Fryer T.D., Cardenas–Blanco A., Smith R., Boros I., Coles J.P., Aigbirhio F.I., Menon D.K., Zaman S.H., Nestor P.J., Holland A.J. The pattern of amyloid accumulation in the brains of adults with Down syndrome. Alzheimers Dement. 2016;12:538–545. - PMC - PubMed
-
- Aylward E.H., Habbak R., Warren A.C., Pulsider M.B., Barta P.E., Jerram M., Pearlson G.D. Cerebellar volume in adults with Down syndrome. Arch. Neurol. 1997;54:209–212. - PubMed
-
- Aylward E.H., Li Q.A., Habbak R., Warren A., Pulsifer M.B., Barta P.E., Jerram M., Pearlson G.D. Basal ganglia volume in adults with Down syndrome. Psychiatry Res. Neuroimaging. 1997;74:73–82. - PubMed
-
- Aylward E.H., Li Q.A., Honeycutt N.A., Warren A.C., Pulsifer M.B., Barta P.E., Chan M.D., Smith P.D., Jerram M., Pearlson G.D. MRI volumes of the hippocampus and amygdala in adults with Down's syndrome with and without dementia. Am. J. Psychiatry. 1999;156:564–568. - PubMed
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
