

Present state and issues in IORT Physics
- PMID: 28193241
- PMCID: PMC5307769
- DOI: 10.1186/s13014-016-0754-z
Present state and issues in IORT Physics
Abstract
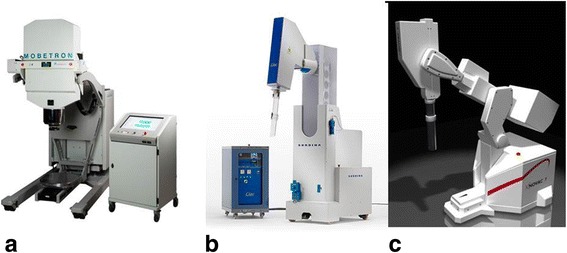
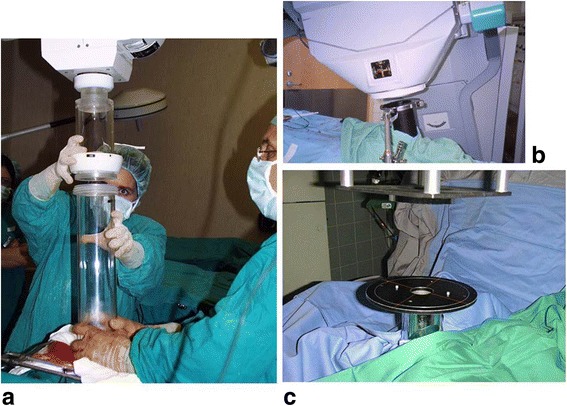
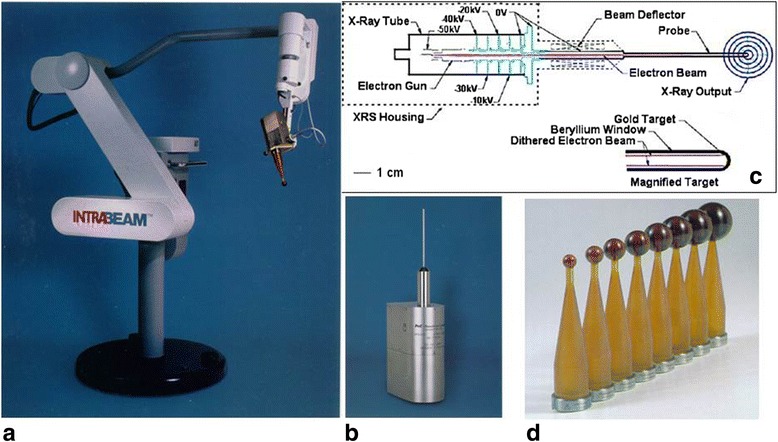
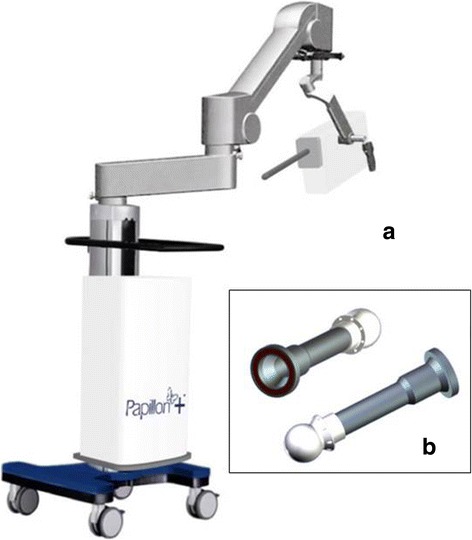
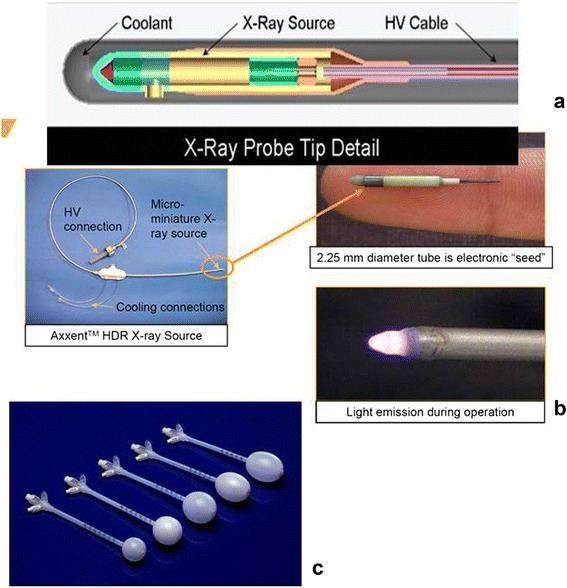
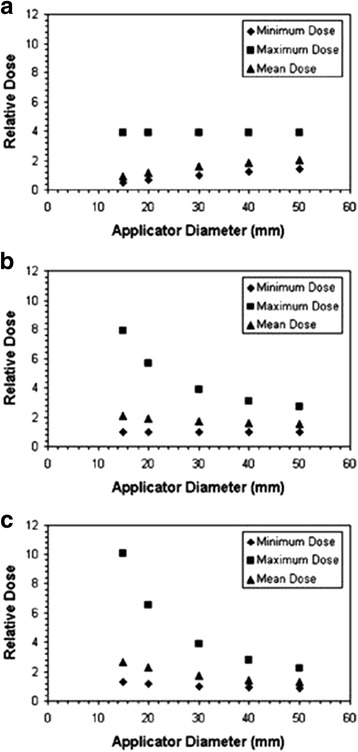
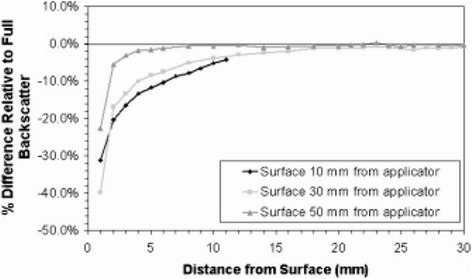
Literature was reviewed to assess the physical aspects governing the present and emerging technologies used in intraoperative radiation therapy (IORT). Three major technologies were identified: treatment with electrons, treatment with external generators of kV X-rays and electronic brachytherapy. Although also used in IORT, literature on brachytherapy with radioactive sources is not systematically reviewed since an extensive own body of specialized literature and reviews exists in this field. A comparison with radioactive sources is made in the use of balloon catheters for partial breast irradiation where these are applied in almost an identical applicator technique as used with kV X-ray sources. The physical constraints of adaption of the dose distribution to the extended target in breast IORT are compared. Concerning further physical issues, the literature on radiation protection, commissioning, calibration, quality assurance (QA) and in-vivo dosimetry of the three technologies was reviewed. Several issues were found in the calibration and the use of dosimetry detectors and phantoms for low energy X-rays which require further investigation. The uncertainties in the different steps of dose determination were estimated, leading to an estimated total uncertainty of around 10-15% for IORT procedures. The dose inhomogeneity caused by the prescription of electrons at 90% and by the steep dose gradient of kV X-rays causes additional deviations from prescription dose which must be considered in the assessment of dose response in IORT.
Figures


References
-
- Palta JR, Biggs PJ, Hazle JD, Huq MS, Dahl RA, Ochran TG, Soen J, Dobelbower RR, Jr, McCullough EC. Intraoperative electron beam radiation therapy: technique, dosimetry, and dose specification: report of task force 48 of the Radiation Therapy Committee, American Association of Physicists in Medicine. Int J Radiat Oncol Biol Phys. 1995;33:725–46. doi: 10.1016/0360-3016(95)00280-C. - DOI - PubMed
-
- Rosi A and Viti V (eds.). Guidelines for quality assurance in intra-operative radiation therapy (English version). Rapporti ISTISAN 03/1 EN 2003 Istituto Superiore di Sanità (Viale Regina Elena, 299 - 00161 Roma)
-
- National Council on Radiation Protection and Measurements . Neutron contamination from medical accelerators. NCRP Report No. 79. Bethesda: NCRP; 1984.
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
