

Incidence of invasive salmonella disease in sub-Saharan Africa: a multicentre population-based surveillance study
- PMID: 28193398
- PMCID: PMC5316558
- DOI: 10.1016/S2214-109X(17)30022-0
Incidence of invasive salmonella disease in sub-Saharan Africa: a multicentre population-based surveillance study
Abstract
Background: Available incidence data for invasive salmonella disease in sub-Saharan Africa are scarce. Standardised, multicountry data are required to better understand the nature and burden of disease in Africa. We aimed to measure the adjusted incidence estimates of typhoid fever and invasive non-typhoidal salmonella (iNTS) disease in sub-Saharan Africa, and the antimicrobial susceptibility profiles of the causative agents.
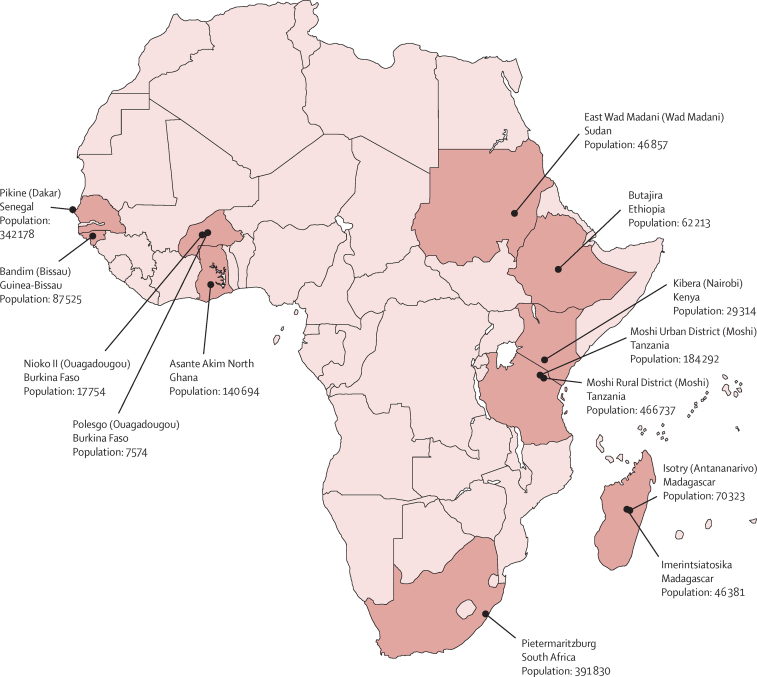
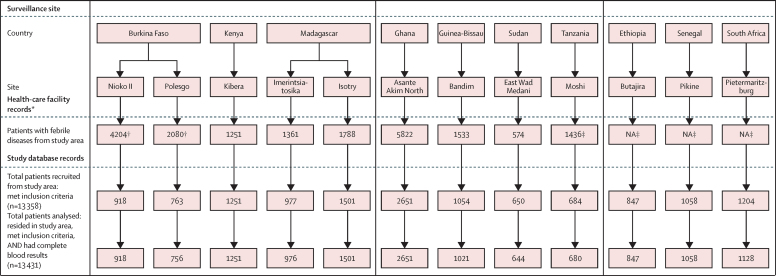
Methods: We established a systematic, standardised surveillance of blood culture-based febrile illness in 13 African sentinel sites with previous reports of typhoid fever: Burkina Faso (two sites), Ethiopia, Ghana, Guinea-Bissau, Kenya, Madagascar (two sites), Senegal, South Africa, Sudan, and Tanzania (two sites). We used census data and health-care records to define study catchment areas and populations. Eligible participants were either inpatients or outpatients who resided within the catchment area and presented with tympanic (≥38·0°C) or axillary temperature (≥37·5°C). Inpatients with a reported history of fever for 72 h or longer were excluded. We also implemented a health-care utilisation survey in a sample of households randomly selected from each study area to investigate health-seeking behaviour in cases of self-reported fever lasting less than 3 days. Typhoid fever and iNTS disease incidences were corrected for health-care-seeking behaviour and recruitment.
Findings: Between March 1, 2010, and Jan 31, 2014, 135 Salmonella enterica serotype Typhi (S Typhi) and 94 iNTS isolates were cultured from the blood of 13 431 febrile patients. Salmonella spp accounted for 33% or more of all bacterial pathogens at nine sites. The adjusted incidence rate (AIR) of S Typhi per 100 000 person-years of observation ranged from 0 (95% CI 0-0) in Sudan to 383 (274-535) at one site in Burkina Faso; the AIR of iNTS ranged from 0 in Sudan, Ethiopia, Madagascar (Isotry site), and South Africa to 237 (178-316) at the second site in Burkina Faso. The AIR of iNTS and typhoid fever in individuals younger than 15 years old was typically higher than in those aged 15 years or older. Multidrug-resistant S Typhi was isolated in Ghana, Kenya, and Tanzania (both sites combined), and multidrug-resistant iNTS was isolated in Burkina Faso (both sites combined), Ghana, Kenya, and Guinea-Bissau.
Interpretation: Typhoid fever and iNTS disease are major causes of invasive bacterial febrile illness in the sampled locations, most commonly affecting children in both low and high population density settings. The development of iNTS vaccines and the introduction of S Typhi conjugate vaccines should be considered for high-incidence settings, such as those identified in this study.
Funding: Bill & Melinda Gates Foundation.
Copyright © 2017 The Author(s). Published by Elsevier Ltd. This is an Open Access article under the CC BY license. Published by Elsevier Ltd.. All rights reserved.
Figures
Comment in
-
Typhoid in Africa and vaccine deployment.Lancet Glob Health. 2017 Mar;5(3):e236-e237. doi: 10.1016/S2214-109X(17)30045-1. Lancet Glob Health. 2017. PMID: 28193381 No abstract available.
References
-
- Langridge GC, Nair S, Wain J. Nontyphoidal Salmonella serovars cause different degrees of invasive disease globally. J Infect Dis. 2009;199:602–603. - PubMed
-
- Mogasale V, Maskery B, Ochiai RL. Burden of typhoid fever in low-income and middle-income countries: a systematic, literature-based update with risk-factor adjustment. Lancet Global Health. 2014;2:e570–e580. - PubMed
Publication types
MeSH terms
Grants and funding
- R01 TW009237/TW/FIC NIH HHS/United States
- U01 AI067854/AI/NIAID NIH HHS/United States
- U01 AI062563/AI/NIAID NIH HHS/United States
- R24 TW007988/TW/FIC NIH HHS/United States
- BB/L018926/1/BB_/Biotechnology and Biological Sciences Research Council/United Kingdom
- WT_/Wellcome Trust/United Kingdom
- P30 AI064518/AI/NIAID NIH HHS/United States
- 001/WHO_/World Health Organization/International
- R01 AI121378/AI/NIAID NIH HHS/United States
- U01 AI069484/AI/NIAID NIH HHS/United States
- BB/J010367/1/BB_/Biotechnology and Biological Sciences Research Council/United Kingdom
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
