

Barriers to Remote Health Interventions for Type 2 Diabetes: A Systematic Review and Proposed Classification Scheme
- PMID: 28193598
- PMCID: PMC5329647
- DOI: 10.2196/jmir.6382
Barriers to Remote Health Interventions for Type 2 Diabetes: A Systematic Review and Proposed Classification Scheme
Abstract
Background: Diabetes self-management involves adherence to healthy daily habits typically involving blood glucose monitoring, medication, exercise, and diet. To support self-management, some providers have begun testing remote interventions for monitoring and assisting patients between clinic visits. Although some studies have shown success, there are barriers to widespread adoption.
Objective: The objective of our study was to identify and classify barriers to adoption of remote health for management of type 2 diabetes.
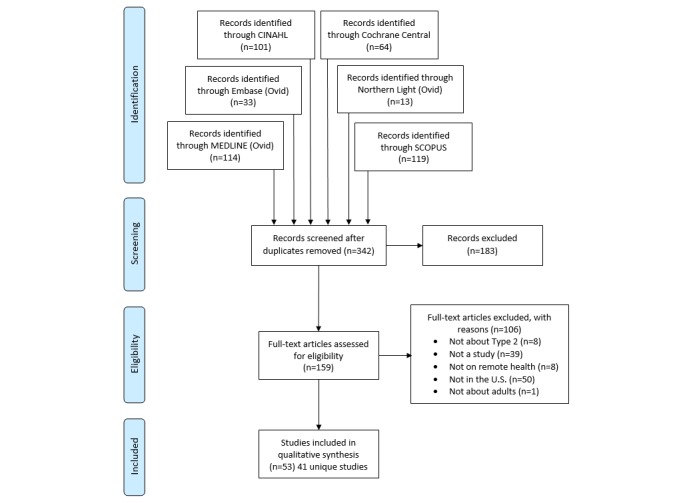
Methods: The following 6 electronic databases were searched for articles published from 2010 to 2015: MEDLINE (Ovid), Embase (Ovid), CINAHL, Cochrane Central, Northern Light Life Sciences Conference Abstracts, and Scopus (Elsevier). The search identified studies involving remote technologies for type 2 diabetes self-management. Reviewers worked in teams of 2 to review and extract data from identified papers. Information collected included study characteristics, outcomes, dropout rates, technologies used, and barriers identified.
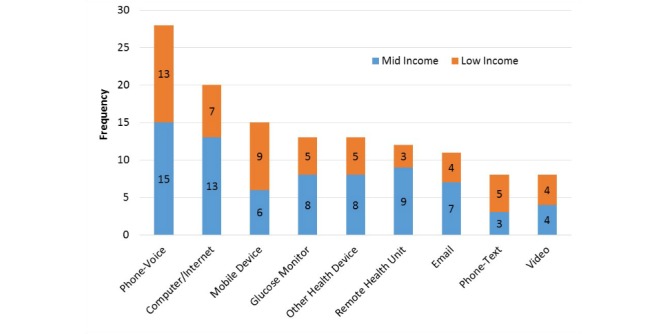
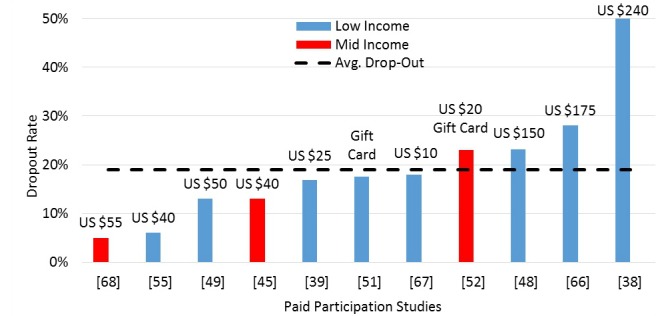
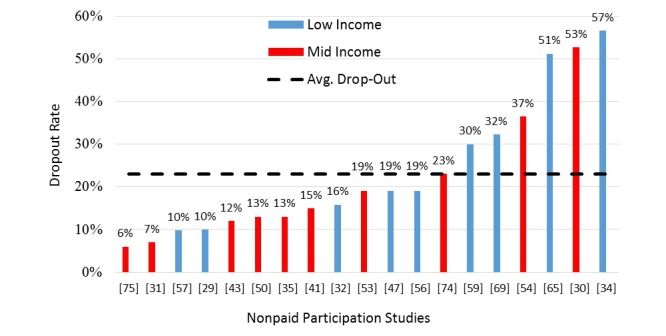
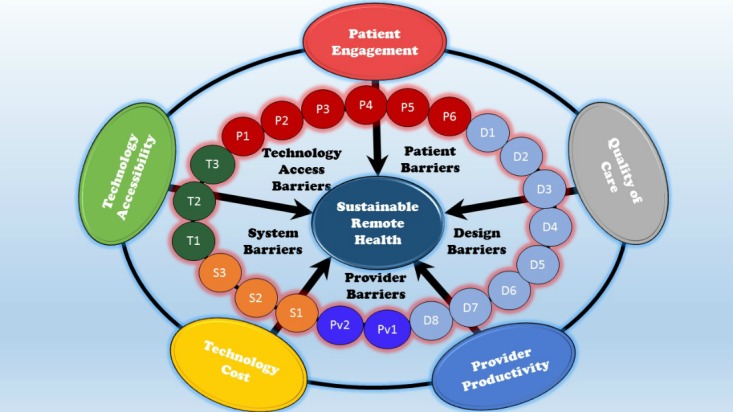
Results: A total of 53 publications on 41 studies met the specified criteria. Lack of data accuracy due to input bias (32%, 13/41), limitations on scalability (24%, 10/41), and technology illiteracy (24%, 10/41) were the most commonly cited barriers. Technology illiteracy was most prominent in low-income populations, whereas limitations on scalability were more prominent in mid-income populations. Barriers identified were applied to a conceptual model of successful remote health, which includes patient engagement, patient technology accessibility, quality of care, system technology cost, and provider productivity. In total, 40.5% (60/148) of identified barrier instances impeded patient engagement, which is manifest in the large dropout rates cited (up to 57%).
Conclusions: The barriers identified represent major challenges in the design of remote health interventions for diabetes. Breakthrough technologies and systems are needed to alleviate the barriers identified so far, particularly those associated with patient engagement. Monitoring devices that provide objective and reliable data streams on medication, exercise, diet, and glucose monitoring will be essential for widespread effectiveness. Additional work is needed to understand root causes of high dropout rates, and new interventions are needed to identify and assist those at the greatest risk of dropout. Finally, future studies must quantify costs and benefits to determine financial sustainability.
Keywords: biomedical technology; diabetes mellitus, type 2; early medical intervention; remote sensing technology; terminology as topic.
©Michelle M Alvarado, Hye-Chung Kum, Karla Gonzalez Coronado, Margaret J Foster, Pearl Ortega, Mark A Lawley. Originally published in the Journal of Medical Internet Research (http://www.jmir.org), 13.02.2017.
Conflict of interest statement
Conflicts of Interest: None declared.
Figures
References
-
- Zhai Y, Zhu W, Cai Y, Sun D, Zhao J. Clinical- and cost-effectiveness of telemedicine in type 2 diabetes mellitus: a systematic review and meta-analysis. Medicine (Baltimore) 2014 Dec;93(28):e312. doi: 10.1097/MD.0000000000000312. http://europepmc.org/abstract/MED/25526482 00005792-201412030-00053 - DOI - PMC - PubMed
-
- van Vugt M, de Wit M, Cleijne WH, Snoek FJ. Use of behavioral change techniques in web-based self-management programs for type 2 diabetes patients: systematic review. J Med Internet Res. 2013 Dec 13;15(12):e279. doi: 10.2196/jmir.2800. http://www.jmir.org/2013/12/e279/ v15i12e279 - DOI - PMC - PubMed
-
- Klonoff DC. The current status of mHealth for diabetes: will it be the next big thing? J Diabetes Sci Technol. 2013 May 01;7(3):749–58. http://europepmc.org/abstract/MED/23759409 - PMC - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
