

Apparent Aortic Stiffness in Children With Pulmonary Arterial Hypertension: Existence of Vascular Interdependency?
- PMID: 28193613
- PMCID: PMC5314208
- DOI: 10.1161/CIRCIMAGING.116.005817
Apparent Aortic Stiffness in Children With Pulmonary Arterial Hypertension: Existence of Vascular Interdependency?
Abstract
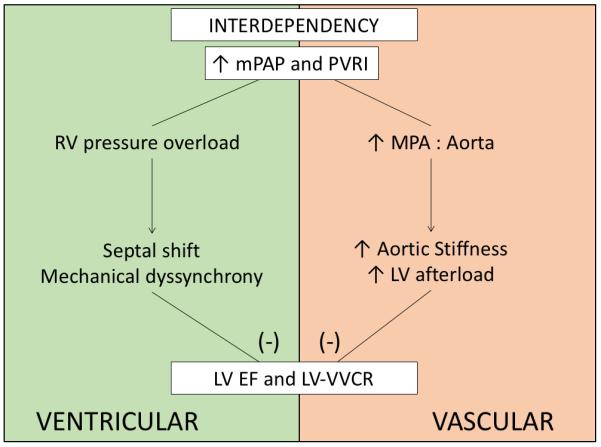
Background: Left ventricular dysfunction, mediated by ventricular interdependence, has been associated with negative outcomes in children with pulmonary arterial hypertension (PAH). Considering the dilation of the pulmonary arteries as a paramount sign of PAH, we hypothesized that the ascending aorta will present signs of apparent stiffness in children with PAH and that this effect may be because of mechanical interaction with the dilated main pulmonary artery (MPA).
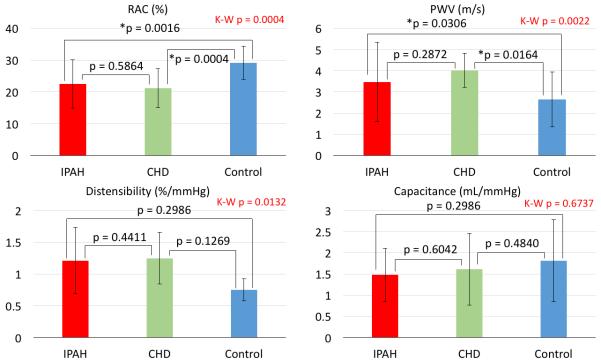
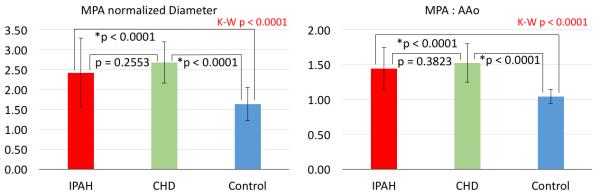
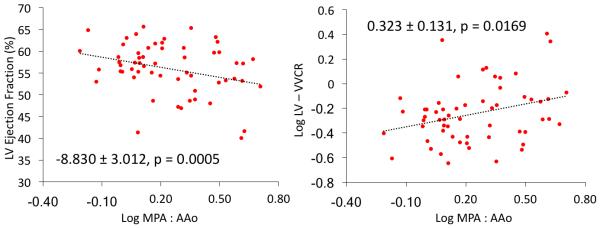
Methods and results: Forty-two children with PAH and 26 age- and size-matched controls underwent comprehensive cardiac magnetic resonance evaluation. Assessment of aortic stiffness was evaluated by measuring pulse wave velocity, aortic strain, and distensibility. Children with PAH had significantly increased pulse wave velocity in the ascending aorta (3.4 versus 2.3 m/s for PAH and controls, respectively; P=0.001) and reduced aortic strain (23% versus 29%; P<0.0001) and distensibility (0.47 versus 0.64%/mm Hg; P=0.02). Indexed MPA diameter correlated with pulse wave velocity (P=0.04) and with aortic strain (P=0.02). The ratio of MPA to aortic size correlated with pulse wave velocity (P=0.0098), strain (P=0.0099), and distensibility (P=0.015). Furthermore, aortic relative area change was associated with left ventricular ejection fraction (P=0.045) and ventricular-vascular coupling ratio (P=0.042).
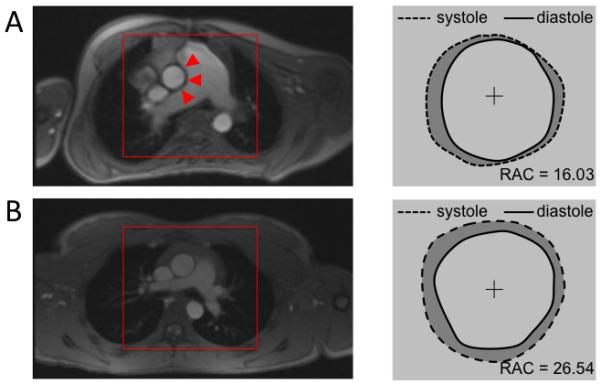
Conclusions: Pediatric PAH patients have increased apparent ascending aortic stiffness, which was strongly associated with the degree of MPA distension. We speculate that distension of the MPA may play a major role in limiting full aortic expansion during systole, which modulates left ventricular performance and impacts systemic hemodynamics in pediatric PAH.
Keywords: aortic stiffness; heart rate; interdependency; pediatric pulmonary hypertension; pulse wave analysis.
© 2017 American Heart Association, Inc.
Figures
Comment in
-
An Unwelcome Embrace: Adverse Pulmonary-Aortic Interactions in Pulmonary Hypertension.Circ Cardiovasc Imaging. 2017 Feb;10(2):e006063. doi: 10.1161/CIRCIMAGING.117.006063. Circ Cardiovasc Imaging. 2017. PMID: 28193614 No abstract available.
References
-
- Abman SH, Hansmann G, Archer SL, Ivy DD, Adatia I, Chung WK, Hanna BD, Rosenzweig EB, Raj JU, Cornfield D, Stenmark KR, Steinhorn R, Thébaud B, Fineman JR, Kuehne T, Feinstein JA, Friedberg MK, Earing M, Barst RJ, Keller RL, Kinsella JP, Mullen M, Deterding R, Kulik T, Mallory G, Humpl T, Wessel DL, American Heart Association Council on Cardiopulmonary, Critical Care, Perioperative and Resuscitation. Council on Clinical Cardiology. Council on Cardiovascular Disease in the Young. Council on Cardiovascular Radiology and Intervention. Council on Cardiovascular Surgery and Anesthesia. the American Thoracic Society Pediatric Pulmonary Hypertension: Guidelines From the American Heart Association and American Thoracic Society. 2015. Circulation. 2015;132:2037–99. - PubMed
-
- Ivy DD, Abman SH, Barst RJ, Berger RMF, Bonnet D, Fleming TR, Haworth SG, Raj JU, Rosenzweig EB, Schulze Neick I, Steinhorn RH, Beghetti M. Pediatric pulmonary hypertension. J Am Coll Cardiol. 2013;62:D117–26. - PubMed
-
- Zijlstra WMH, Douwes JM, Rosenzweig EB, Schokker S, Krishnan U, Roofthooft MTR, Miller-Reed K, Hillege HL, Ivy DD, Berger RMF. Survival differences in pediatric pulmonary arterial hypertension: Clues to a better understanding of outcome and optimal treatment strategies. J Am Coll Cardiol. 2014;63:2159–2169. - PubMed
-
- Vonk-Noordegraaf A, Haddad F, Chin KM, Forfia PR, Kawut SM, Lumens J, Naeije R, Newman J, Oudiz RJ, Provencher S, Torbicki A, Voelkel NF, Hassoun PM. Right heart adaptation to pulmonary arterial hypertension: physiology and pathobiology. J Am Coll Cardiol. 2013;62:D22–33. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
