

Antimicrobial Resistance of Escherichia coli Urinary Isolates in the Veterans Affairs Health Care System
- PMID: 28193660
- PMCID: PMC5404570
- DOI: 10.1128/AAC.02236-16
Antimicrobial Resistance of Escherichia coli Urinary Isolates in the Veterans Affairs Health Care System
Abstract
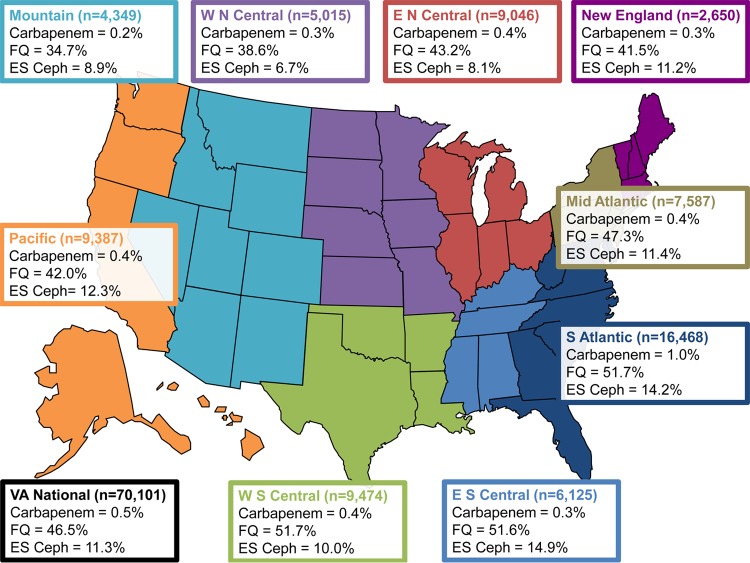
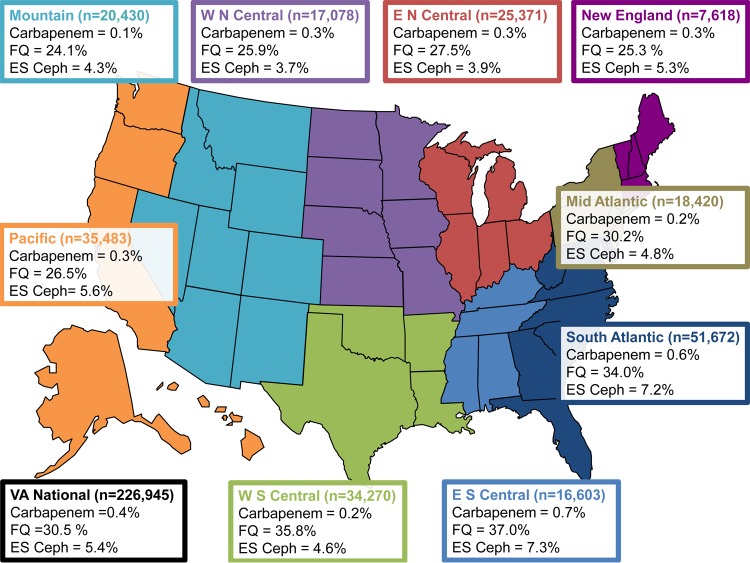
We reviewed data for almost 300,000 clinical Escherichia coli urinary isolates (collected in 2009 through 2013) from 127 inpatient and outpatient facilities, to assess antibiotic resistance among Veterans Affairs health care system patients using Clinical and Laboratory Standards Institute and Centers for Disease Control and Prevention National Healthcare Safety Network definitions or guidance. Rates of resistance to amoxicillin or ampicillin/β-lactamase inhibitors were approximately 40% and rates of resistance to fluoroquinolones and trimethoprim-sulfamethoxazole approached 30%. Rates of resistance to nitrofurantoin, antipseudomonal penicillin/β-lactamase inhibitors, and carbapenems remained less than 10%. The percentage of isolates that were considered multidrug resistant varied (4% to 37%), depending on the definitions used.
Keywords: Escherichia coli; resistance; urinary tract infection.
Copyright © 2017 American Society for Microbiology.
Figures
References
-
- Hooton TM, Bradley SF, Cardenas DD, Colgan R, Geerlings SE, Rice JC, Saint S, Schaeffer AJ, Tambayh PA, Tenke P, Nicolle LE. 2010. Diagnosis, prevention, and treatment of catheter-associated urinary tract infection in adults: 2009 International Clinical Practice Guidelines from the Infectious Diseases Society of America. Clin Infect Dis 50:625–663. doi: 10.1086/650482. - DOI - PubMed
-
- Gupta K, Hooton TM, Naber KG, Wullt B, Colgan R, Miller LG, Moran GJ, Nicolle LE, Raz R, Schaeffer AJ, Soper DE. 2011. International clinical practice guidelines for the treatment of acute uncomplicated cystitis and pyelonephritis in women: a 2010 update by the Infectious Diseases Society of America and the European Society for Microbiology and Infectious Diseases. Clin Infect Dis 52:e103–e120. doi: 10.1093/cid/ciq257. - DOI - PubMed
-
- Clinical and Laboratory Standards Institute. 2014. Analysis and presentation of cumulative antimicrobial susceptibility test data; approved guideline—4th ed. CLSI document M39-A4 Clinical and Laboratory Standards Institute, Wayne, PA.
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
