

Results from a Patient-Based Health Education Intervention in Reducing Antibiotic Use for Acute Upper Respiratory Tract Infections in the Private Sector Primary Care Setting in Singapore
- PMID: 28193663
- PMCID: PMC5404603
- DOI: 10.1128/AAC.02257-16
Results from a Patient-Based Health Education Intervention in Reducing Antibiotic Use for Acute Upper Respiratory Tract Infections in the Private Sector Primary Care Setting in Singapore
Abstract
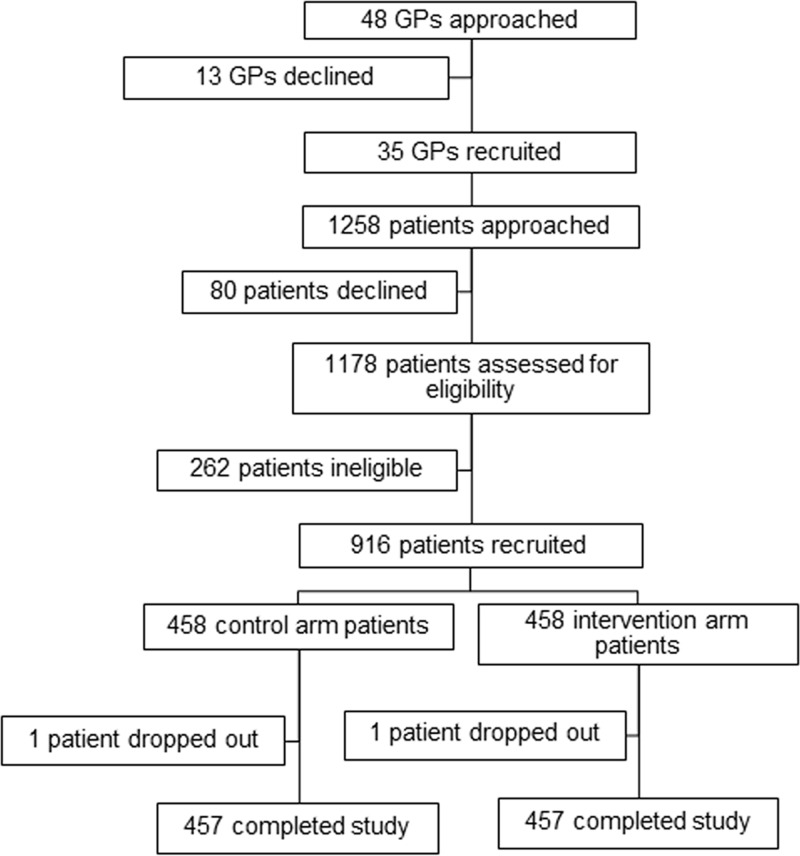
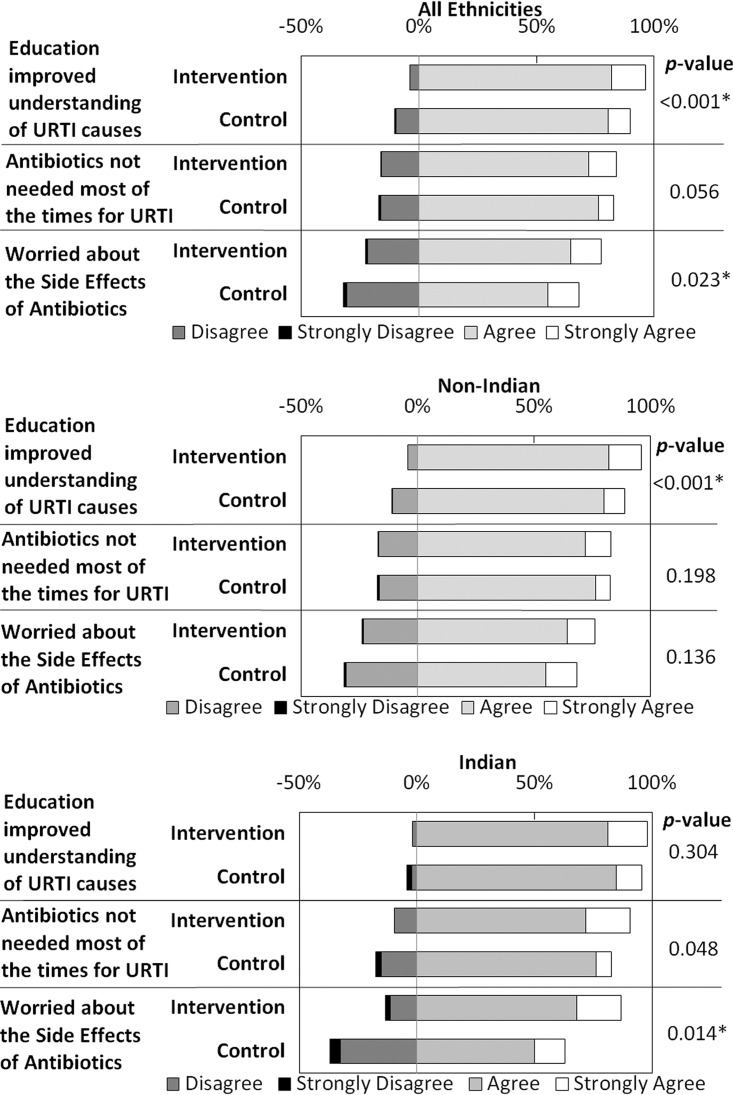
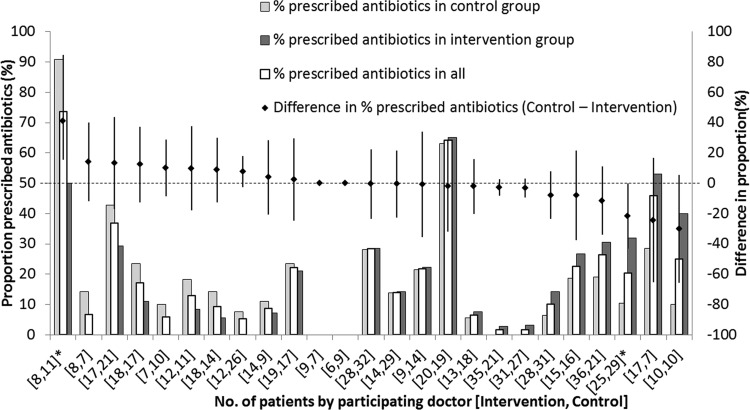
We investigated the efficacy of patient-targeted education in reducing antibiotic prescriptions for upper respiratory tract infections (URTIs) among adults in the private primary care setting in Singapore. Our randomized controlled trial enrolled patients aged 21 years and above presenting at general practitioner (GP) clinics with URTI symptoms for 7 days or less. Intervention arm patients were verbally educated via pamphlets about the etiology of URTIs, the role of antibiotics in treating URTIs, and the consequences of inappropriate antibiotic use. Control arm patients were educated on influenza vaccinations. Both arms were compared regarding the proportions prescribed antibiotics and the patients' postconsultation views. A total of 914 patients consulting 35 doctors from 24 clinics completed the study (457 in each arm). The demographics of patients in both arms were similar, and 19.1% were prescribed an antibiotic, but this varied from 0% to 70% for individual GPs. The intervention did not significantly reduce antibiotic prescriptions (odds ratio [OR], 1.20; 95% confidence interval [CI], 0.83-1.73) except in patients of Indian ethnicity (OR, 0.28; 95% CI, 0.09-0.93). Positive associations between the intervention and the view that antibiotics were not needed most of the time for URTIs (P = 0.047) and on being worried about the side effects of antibiotics (P = 0.018) were restricted to the Indian subgroup. GPs in limited liability partnerships or clinic chains prescribed less (OR, 0.36; 95% CI, 0.14 to 0.92), while certain inappropriate patient responses were associated with the receipt of antibiotics. Follow-up studies to investigate differences in responses to educational programs between ethnicities and to explore GP-targeted interventions are recommended.
Keywords: antibiotics; antimicrobial stewardship; intervention; upper respiratory tract infection.
Copyright © 2017 Lee et al.
Figures
References
-
- World Health Organization. 2014. Antimicrobial resistance: global report on surveillance. World Health Organization, Geneva, Switzerland.
-
- Sng QS. 2011. Primary care survey 2010. Profile of primary care patients. Ministry of Health, Singapore.
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
