

Molecular classification of urothelial carcinoma: global mRNA classification versus tumour-cell phenotype classification
- PMID: 28195647
- PMCID: PMC5413843
- DOI: 10.1002/path.4886
Molecular classification of urothelial carcinoma: global mRNA classification versus tumour-cell phenotype classification
Abstract
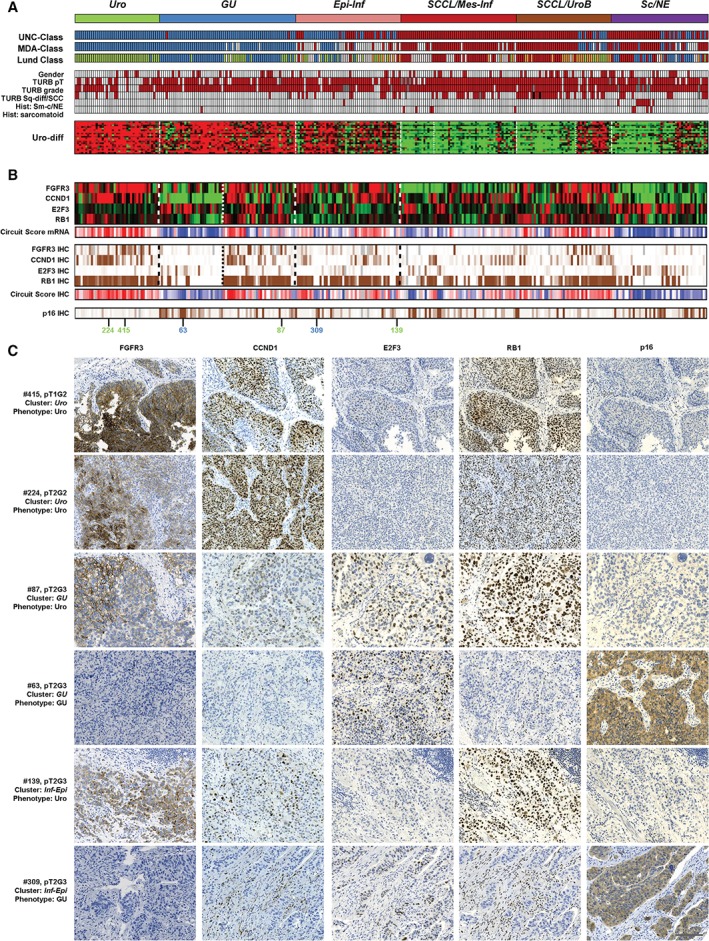
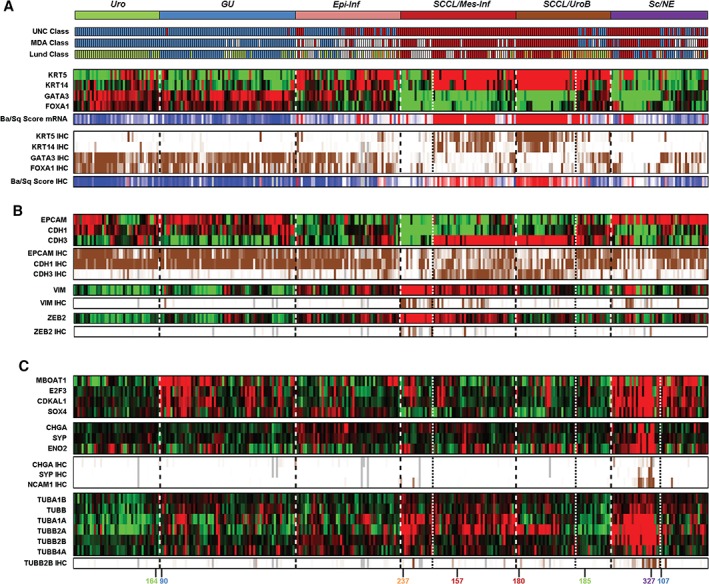
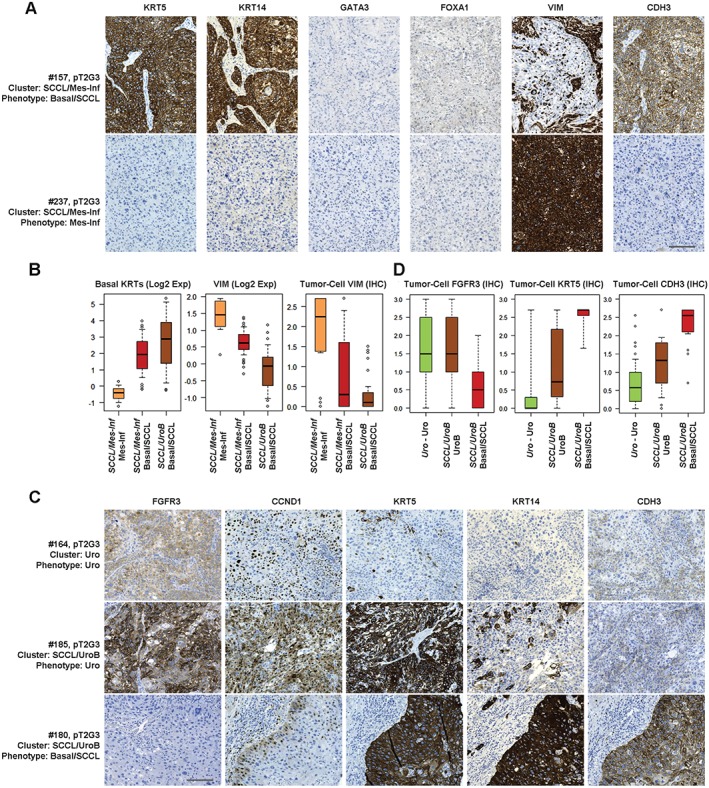
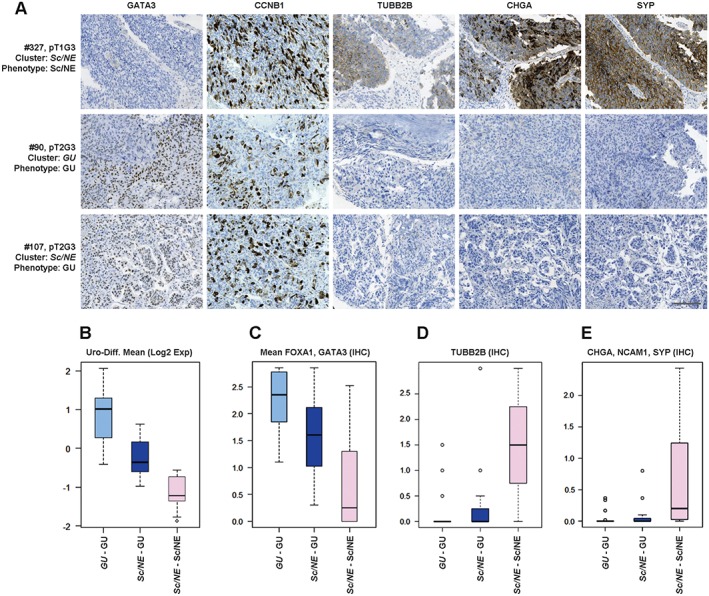
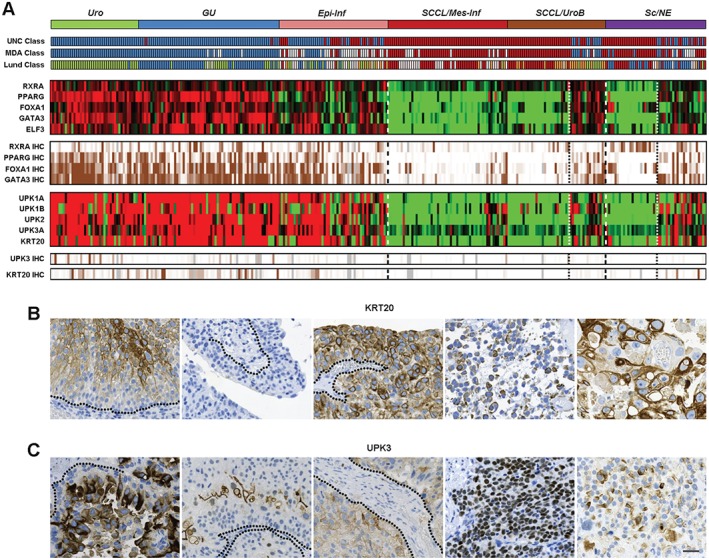
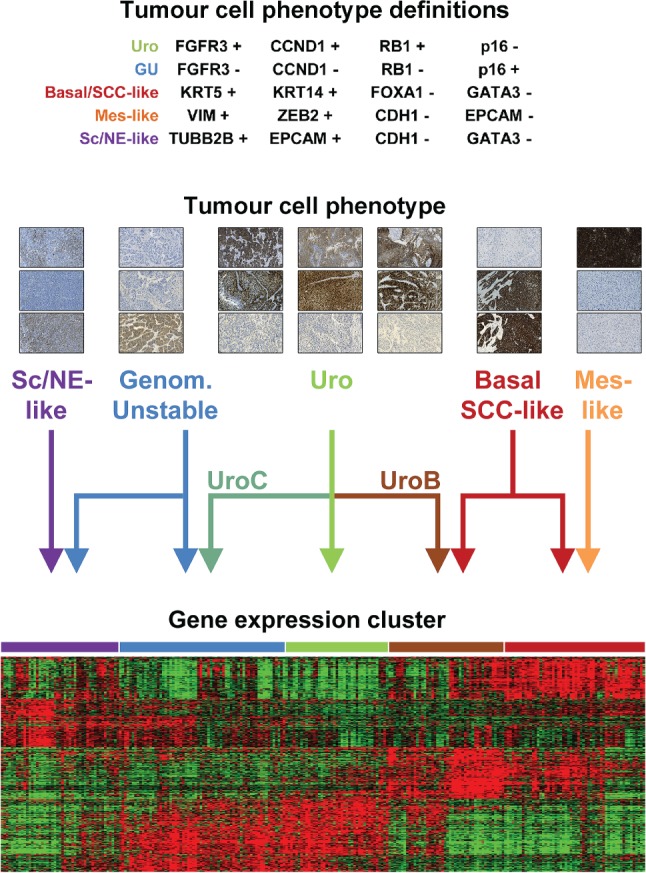
Global mRNA expression analysis is efficient for phenotypic profiling of tumours, and has been used to define molecular subtypes for almost every major tumour type. A key limitation is that most tumours are communities of both tumour and non-tumour cells. This problem is particularly pertinent for analysis of advanced invasive tumours, which are known to induce major changes and responses in both the tumour and the surrounding tissue. To identify bladder cancer tumour-cell phenotypes and compare classification by tumour-cell phenotype with classification by global gene expression analysis, we analysed 307 advanced bladder cancers (cystectomized) both by genome gene expression analysis and by immunohistochemistry with antibodies for 28 proteins. According to systematic analysis of gene and protein expression data, focusing on key molecular processes, we describe five tumour-cell phenotypes of advanced urothelial carcinoma: urothelial-like, genomically unstable, basal/SCC-like, mesenchymal-like, and small-cell/neuroendocrine-like. We provide molecular pathological definitions for each subtype. Tumours expressing urothelial differentiation factors show inconsistent and abnormal protein expression of terminal differentiation markers, suggesting pseudo-differentiation. Cancers with different tumour-cell phenotypes may co-cluster (converge), and cases with identical tumour-cell phenotypes may cluster apart (diverge), in global mRNA analyses. This divergence/convergence suggests that broad global commonalities related to the invasive process may exist between muscle-invasive tumours regardless of specific tumour-cell phenotype. Hence, there is a systematic disagreement in subtype classification determined by global mRNA profiling and by immunohistochemical profiling at the tumour-cell level. We suggest that a combination of molecular pathology (tumour-cell phenotype) and global mRNA profiling (context) is required for adequate subtype classification of muscle-invasive bladder cancer. © 2017 The Authors. The Journal of Pathology published by John Wiley & Sons Ltd on behalf of Pathological Society of Great Britain and Ireland.
Keywords: bladder cancer; molecular classification; pseudo-differentiation; tumour-cell phenotypes.
© 2017 The Authors. The Journal of Pathology published by John Wiley & Sons Ltd on behalf of Pathological Society of Great Britain and Ireland.
Figures
Comment in
-
Re: Molecular Classification of Urothelial Carcinoma: Global mRNA Classification Versus Tumour-cell Phenotype Classification.Eur Urol. 2018 May;73(5):809-810. doi: 10.1016/j.eururo.2017.12.011. Epub 2017 Dec 19. Eur Urol. 2018. PMID: 29273405 No abstract available.
References
-
- Hayes DN, Monti S, Parmigiani G, et al Gene expression profiling reveals reproducible human lung adenocarcinoma subtypes in multiple independent patient cohorts. J Clin Oncol 2006; 24 : 5079–5090. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Molecular Biology Databases
Research Materials
