

Assessment of Surgical Learning Curves in Transoral Robotic Surgery for Squamous Cell Carcinoma of the Oropharynx
- PMID: 28196200
- PMCID: PMC5614443
- DOI: 10.1001/jamaoto.2016.4132
Assessment of Surgical Learning Curves in Transoral Robotic Surgery for Squamous Cell Carcinoma of the Oropharynx
Abstract
Importance: Transoral robotic surgery (TORS) is increasingly employed as a treatment option for squamous cell carcinoma of the oropharynx (OPSCC). Measures of surgical learning curves are needed particularly as clinical trials using this technology continue to evolve.
Objective: To assess learning curves for the oncologic TORS surgeon and to identify the number of cases needed to identify the learning phase.
Design, setting, and participants: A retrospective review of all patients who underwent TORS for OPSCC at the University of Pittsburgh Medical Center between March 2010 and March 2016. Cases were excluded for involvement of a subsite outside of the oropharynx, for nonmalignant abnormality or nonsquamous histology, unknown primary, no tumor in the main specimen, free flap reconstruction, and for an inability to define margin status.
Exposures: Transoral robotic surgery for OPSCC.
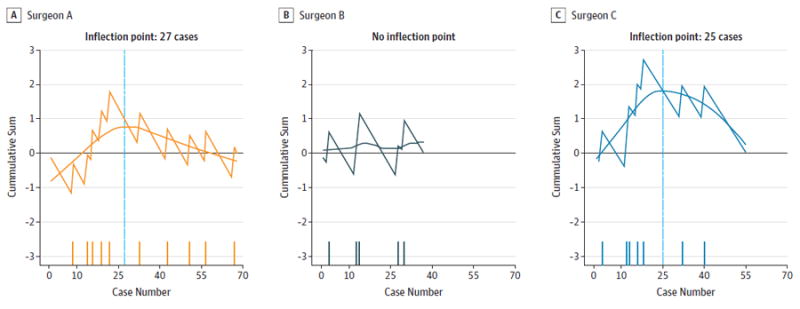
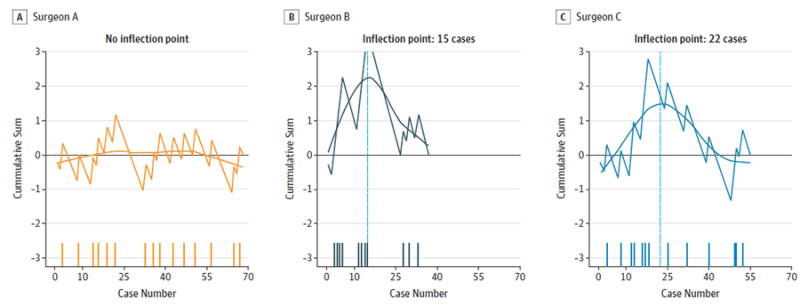
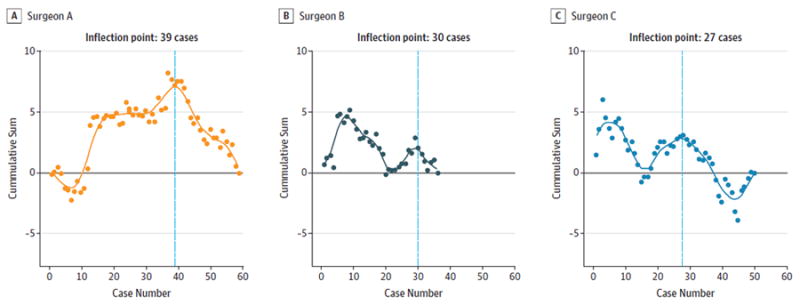
Main outcomes and measures: Primary learning measures defined by the authors include the initial and final margin status and time to resection of main surgical specimen. A cumulative sum learning curve was developed for each surgeon for each of the study variables. The inflection point of each surgeon's curve was considered to be the point signaling the completion of the learning phase.
Results: There were 382 transoral robotic procedures identified. Of 382 cases, 160 met our inclusion criteria: 68 for surgeon A, 37 for surgeon B, and 55 for surgeon C. Of the 160 included patients, 125 were men and 35 were women. The mean (SD) age of participants was 59.4 (9.5) years. Mean (SD) time to resection including robot set-up was 79 (36) minutes. The inflection points for the final margin status learning curves were 27 cases (surgeon A) and 25 cases (surgeon C). There was no inflection point for surgeon B for final margin status. Inflection points for mean time to resection were: 39 cases (surgeon A), 30 cases (surgeon B), and 27 cases (surgeon C).
Conclusions and relevance: Using metrics of positive margin rate and time to resection of the main surgical specimen, the learning curve for TORS for OPSCC is surgeon-specific. Inflection points for most learning curves peak between 20 and 30 cases.
Conflict of interest statement
Figures
References
-
- Weinstein GS, O’Malley BW, Jr, Snyder W, Sherman E, Quon H. Transoral robotic surgery: radical tonsillectomy. Arch Otolaryngol Head Neck Surg. 2007;133(12):1220–1226. - PubMed
-
- Chen MM, Roman SA, Kraus DH, Sosa JA, Judson BL. Transoral Robotic Surgery: A Population-Level Analysis. Otolaryngol Head Neck Surg. 2014;150(6):968–975. - PubMed
-
- Weinstein GS, O’Malley BW, Jr, Magnuson JS, et al. Transoral robotic surgery: a multicenter study to assess feasibility, safety, and surgical margins. Laryngoscope. 2012;122(8):1701–1707. - PubMed
-
- Gross ND, Holsinger FC, Magnuson JS, et al. Robotics in otolaryngology and head and neck surgery: recommendations for training and credentialing: A report of the 2015 AHNS education committee, AAO-HNS robotic task force and AAO-HNS sleep disorders committee. Head Neck. 2016;38(suppl 1):E151–E158. - PMC - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Miscellaneous
