

Genetic Association of Waist-to-Hip Ratio With Cardiometabolic Traits, Type 2 Diabetes, and Coronary Heart Disease
- PMID: 28196256
- PMCID: PMC5571980
- DOI: 10.1001/jama.2016.21042
Genetic Association of Waist-to-Hip Ratio With Cardiometabolic Traits, Type 2 Diabetes, and Coronary Heart Disease
Abstract
Importance: In observational studies, abdominal adiposity has been associated with type 2 diabetes and coronary heart disease (CHD). Whether these associations represent causal relationships remains uncertain.
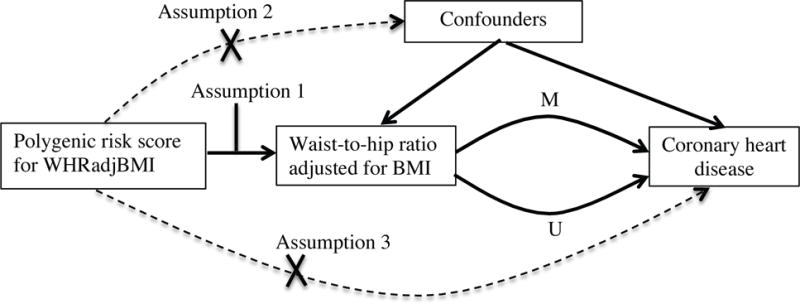
Objective: To test the association of a polygenic risk score for waist-to-hip ratio (WHR) adjusted for body mass index (BMI), a measure of abdominal adiposity, with type 2 diabetes and CHD through the potential intermediates of blood lipids, blood pressure, and glycemic phenotypes.
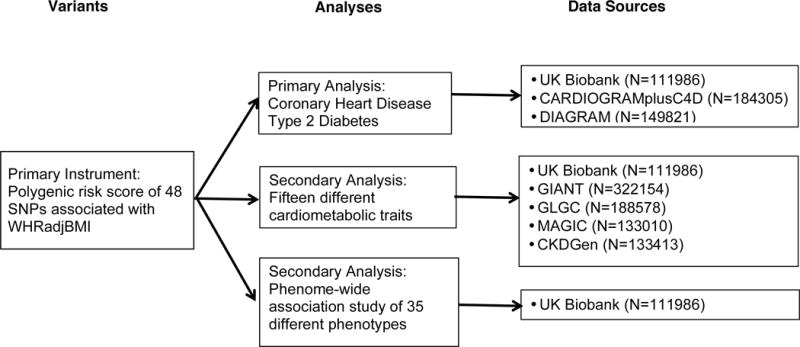
Design, setting, and participants: A polygenic risk score for WHR adjusted for BMI, a measure of genetic predisposition to abdominal adiposity, was constructed with 48 single-nucleotide polymorphisms. The association of this score with cardiometabolic traits, type 2 diabetes, and CHD was tested in a mendelian randomization analysis that combined case-control and cross-sectional data sets. Estimates for cardiometabolic traits were based on a combined data set consisting of summary results from 4 genome-wide association studies conducted from 2007 to 2015, including up to 322 154 participants, as well as individual-level, cross-sectional data from the UK Biobank collected from 2007-2011, including 111 986 individuals. Estimates for type 2 diabetes and CHD were derived from summary statistics of 2 separate genome-wide association studies conducted from 2007 to 2015 and including 149 821 individuals and 184 305 individuals, respectively, combined with individual-level data from the UK Biobank.
Exposures: Genetic predisposition to increased WHR adjusted for BMI.
Main outcomes and measures: Type 2 diabetes and CHD.
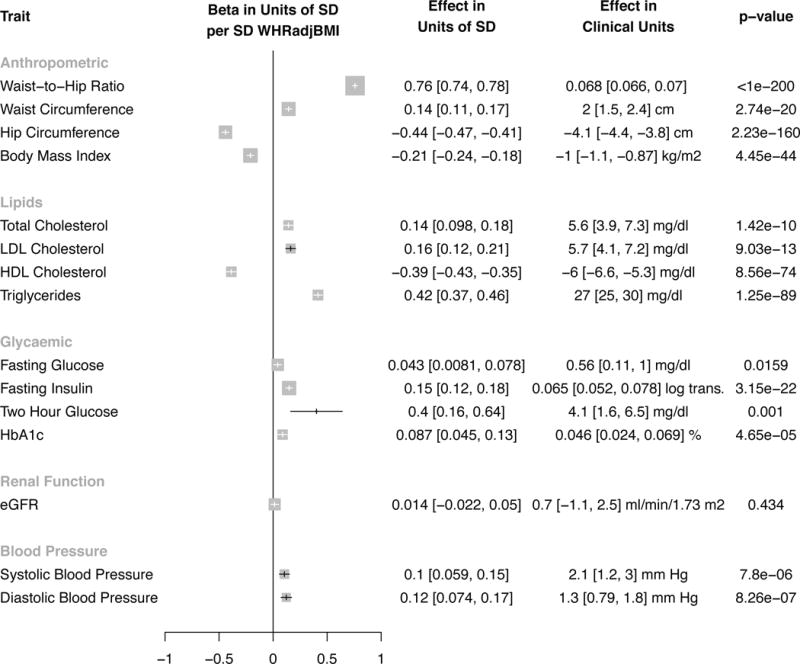
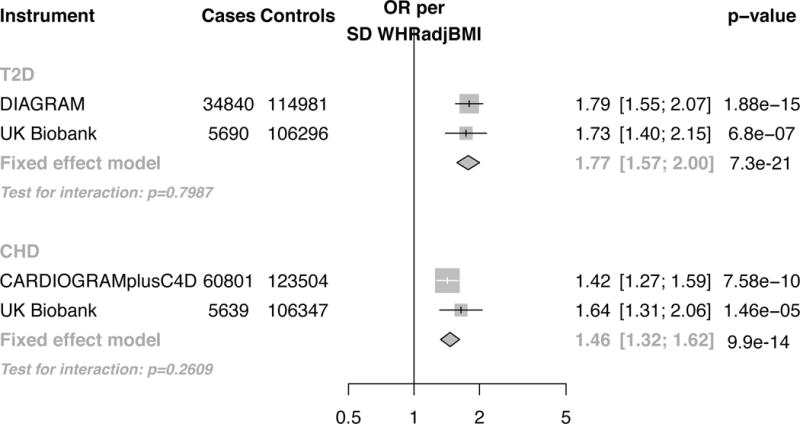
Results: Among 111 986 individuals in the UK Biobank, the mean age was 57 (SD, 8) years, 58 845 participants (52.5%) were women, and mean WHR was 0.875. Analysis of summary-level genome-wide association study results and individual-level UK Biobank data demonstrated that a 1-SD increase in WHR adjusted for BMI mediated by the polygenic risk score was associated with 27-mg/dL higher triglyceride levels, 4.1-mg/dL higher 2-hour glucose levels, and 2.1-mm Hg higher systolic blood pressure (each P < .001). A 1-SD genetic increase in WHR adjusted for BMI was also associated with a higher risk of type 2 diabetes (odds ratio, 1.77 [95% CI, 1.57-2.00]; absolute risk increase per 1000 participant-years, 6.0 [95% CI, CI, 4.4-7.8]; number of participants with type 2 diabetes outcome, 40 530) and CHD (odds ratio, 1.46 [95% CI, 1.32-1.62]; absolute risk increase per 1000 participant-years, 1.8 [95% CI, 1.3-2.4]; number of participants with CHD outcome, 66 440).
Conclusions and relevance: A genetic predisposition to higher waist-to-hip ratio adjusted for body mass index was associated with increased risk of type 2 diabetes and coronary heart disease. These results provide evidence supportive of a causal association between abdominal adiposity and these outcomes.
Figures
Comment in
-
When Will Mendelian Randomization Become Relevant for Clinical Practice and Public Health?JAMA. 2017 Feb 14;317(6):589-591. doi: 10.1001/jama.2016.21189. JAMA. 2017. PMID: 28196238 No abstract available.
-
Adipose tissue: Apple or pear - waist-to-hip ratio and the risk of CHD and T2DM.Nat Rev Endocrinol. 2017 Apr;13(4):187. doi: 10.1038/nrendo.2017.26. Epub 2017 Mar 3. Nat Rev Endocrinol. 2017. PMID: 28256627 No abstract available.
-
Genetic Predisposition to Abdominal Adiposity and Cardiometabolic Risk.JAMA. 2017 Jun 13;317(22):2334. doi: 10.1001/jama.2017.5041. JAMA. 2017. PMID: 28609526 No abstract available.
References
-
- Seidell JC, Björntorp P, Sjöström L, Sannerstedt R, Krotkiewski M, Kvist H. Regional distribution of muscle and fat mass in men–new insight into the risk of abdominal obesity using computed tomography. Int J Obes. 1989;13(3):289–303. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
