

Association of Coronary Artery Calcium in Adults Aged 32 to 46 Years With Incident Coronary Heart Disease and Death
- PMID: 28196265
- PMCID: PMC5397328
- DOI: 10.1001/jamacardio.2016.5493
Association of Coronary Artery Calcium in Adults Aged 32 to 46 Years With Incident Coronary Heart Disease and Death
Abstract
Importance: Coronary artery calcium (CAC) is associated with coronary heart disease (CHD) and cardiovascular disease (CVD); however, prognostic data on CAC are limited in younger adults.
Objective: To determine if CAC in adults aged 32 to 46 years is associated with incident clinical CHD, CVD, and all-cause mortality during 12.5 years of follow-up.
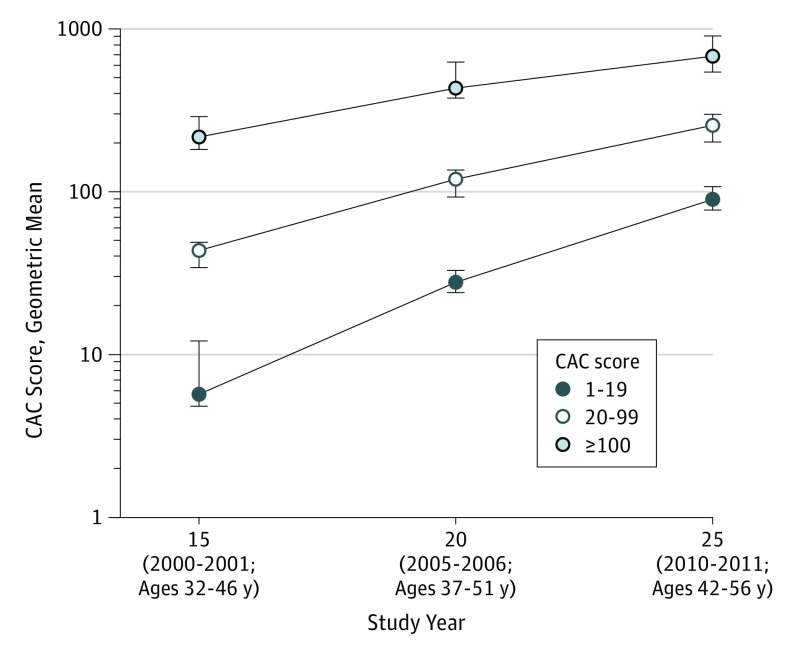
Design, setting, and participants: The Coronary Artery Risk Development in Young Adults (CARDIA) Study is a prospective community-based study that recruited 5115 black and white participants aged 18 to 30 years from March 25, 1985, to June 7, 1986. The cohort has been under surveillance for 30 years, with CAC measured 15 (n = 3043), 20 (n = 3141), and 25 (n = 3189) years after recruitment. The mean follow-up period for incident events was 12.5 years, from the year 15 computed tomographic scan through August 31, 2014.
Main outcomes and measures: Incident CHD included fatal or nonfatal myocardial infarction, acute coronary syndrome without myocardial infarction, coronary revascularization, or CHD death. Incident CVD included CHD, stroke, heart failure, and peripheral arterial disease. Death included all causes. The probability of developing CAC by age 32 to 56 years was estimated using clinical risk factors measured 7 years apart between ages 18 and 38 years.
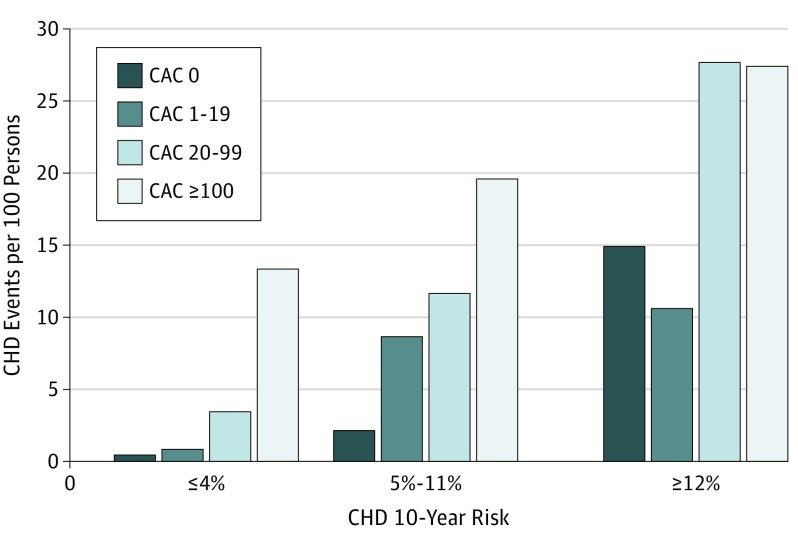
Results: At year 15 of the study among 3043 participants (mean [SD] age, 40.3 [3.6] years; 1383 men and 1660 women), 309 individuals (10.2%) had CAC, with a geometric mean Agatston score of 21.6 (interquartile range, 17.3-26.8). Participants were followed up for 12.5 years, with 57 incident CHD events and 108 incident CVD events observed. After adjusting for demographics, risk factors, and treatments, those with any CAC experienced a 5-fold increase in CHD events (hazard ratio [HR], 5.0; 95% CI, 2.8-8.7) and 3-fold increase in CVD events (HR, 3.0; 95% CI, 1.9-4.7). Within CAC score strata of 1-19, 20-99, and 100 or more, the HRs for CHD were 2.6 (95% CI, 1.0-5.7), 5.8 (95% CI, 2.6-12.1), and 9.8 (95% CI, 4.5-20.5), respectively. A CAC score of 100 or more had an incidence of 22.4 deaths per 100 participants (HR, 3.7; 95% CI, 1.5-10.0); of the 13 deaths in participants with a CAC score of 100 or more, 10 were adjudicated as CHD events. Risk factors for CVD in early adult life identified those above the median risk for developing CAC and, if applied, in a selective CAC screening strategy could reduce the number of people screened for CAC by 50% and the number imaged needed to find 1 person with CAC from 3.5 to 2.2.
Conclusions and relevance: The presence of CAC among individuals aged between 32 and 46 years was associated with increased risk of fatal and nonfatal CHD during 12.5 years of follow-up. A CAC score of 100 or more was associated with early death. Adults younger than 50 years with any CAC, even with very low scores, identified on a computed tomographic scan are at elevated risk of clinical CHD, CVD, and death. Selective use of screening for CAC might be considered in individuals with risk factors in early adulthood to inform discussions about primary prevention.
Conflict of interest statement
Figures
Comment in
-
Screening for Coronary Artery Disease at an Earlier Age.JAMA Cardiol. 2017 Apr 1;2(4):357-358. doi: 10.1001/jamacardio.2016.5552. JAMA Cardiol. 2017. PMID: 28196189 No abstract available.
Similar articles
-
Spatially Weighted Coronary Artery Calcium Score and Coronary Heart Disease Events in the Multi-Ethnic Study of Atherosclerosis.Circ Cardiovasc Imaging. 2021 Jan;14(1):e011981. doi: 10.1161/CIRCIMAGING.120.011981. Epub 2021 Jan 19. Circ Cardiovasc Imaging. 2021. PMID: 33461306 Free PMC article.
-
Impact of coronary artery calcium on mortality and cardiovascular events in metabolic syndrome and diabetes among younger adults.Eur J Prev Cardiol. 2024 Apr 18;31(6):744-753. doi: 10.1093/eurjpc/zwae039. Eur J Prev Cardiol. 2024. PMID: 38323650
-
Greater Volume but not Higher Density of Abdominal Aortic Calcium Is Associated With Increased Cardiovascular Disease Risk: MESA (Multi-Ethnic Study of Atherosclerosis).Circ Cardiovasc Imaging. 2016 Nov;9(11):e005138. doi: 10.1161/CIRCIMAGING.116.005138. Circ Cardiovasc Imaging. 2016. PMID: 27903540 Free PMC article.
-
Association of polygenic risk scores with incident atherosclerotic cardiovascular disease events among individuals with coronary artery calcium score of zero: The multi-ethnic study of atherosclerosis.Prog Cardiovasc Dis. 2022 Sep-Oct;74:19-27. doi: 10.1016/j.pcad.2022.08.003. Epub 2022 Aug 8. Prog Cardiovasc Dis. 2022. PMID: 35952728 Free PMC article. Review.
-
Beyond the Agatston calcium score: role of calcium density and other calcified plaque markers for cardiovascular disease prediction.Curr Opin Cardiol. 2025 Jan 1;40(1):56-62. doi: 10.1097/HCO.0000000000001185. Epub 2024 Oct 9. Curr Opin Cardiol. 2025. PMID: 39445716 Review.
Cited by
-
Evolution of Coronary Calcium Screening for Assessment of Atherosclerotic Cardiovascular Disease Risk and Role in Preventive Cardiology.Curr Atheroscler Rep. 2022 Dec;24(12):949-957. doi: 10.1007/s11883-022-01073-z. Epub 2022 Nov 14. Curr Atheroscler Rep. 2022. PMID: 36374366 Free PMC article. Review.
-
Statins and Atherosclerotic Lesion Microcalcification: A New Mechanism for Plaque Stability?Arterioscler Thromb Vasc Biol. 2021 Apr;41(4):1306-1308. doi: 10.1161/ATVBAHA.121.315949. Epub 2021 Mar 24. Arterioscler Thromb Vasc Biol. 2021. PMID: 33760629 Free PMC article. No abstract available.
-
Exposure to Neighborhood-Level Racial Residential Segregation in Young Adulthood to Midlife and Incident Subclinical Atherosclerosis in Black Adults: The Coronary Artery Risk Development in Young Adults Study.Circ Cardiovasc Qual Outcomes. 2022 Feb;15(2):e007986. doi: 10.1161/CIRCOUTCOMES.121.007986. Epub 2022 Feb 2. Circ Cardiovasc Qual Outcomes. 2022. PMID: 35105173 Free PMC article.
-
The Implication of Coronary Artery Calcium Testing for Cardiovascular Disease Prevention and Diabetes.Endocrinol Metab (Seoul). 2017 Mar;32(1):47-57. doi: 10.3803/EnM.2017.32.1.47. Endocrinol Metab (Seoul). 2017. PMID: 28345316 Free PMC article. Review.
-
The Miami Heart Study (MiHeart) at Baptist Health South Florida, A prospective study of subclinical cardiovascular disease and emerging cardiovascular risk factors in asymptomatic young and middle-aged adults: The Miami Heart Study: Rationale and Design.Am J Prev Cardiol. 2021 May 28;7:100202. doi: 10.1016/j.ajpc.2021.100202. eCollection 2021 Sep. Am J Prev Cardiol. 2021. PMID: 34611641 Free PMC article.
References
-
- Detrano R, Guerci AD, Carr JJ, et al. . Coronary calcium as a predictor of coronary events in four racial or ethnic groups. N Engl J Med. 2008;358(13):1336-1345. - PubMed
-
- Elias-Smale SE, Proença RV, Koller MT, et al. . Coronary calcium score improves classification of coronary heart disease risk in the elderly: the Rotterdam study. J Am Coll Cardiol. 2010;56(17):1407-1414. - PubMed
-
- Vliegenthart R, Oudkerk M, Hofman A, et al. . Coronary calcification improves cardiovascular risk prediction in the elderly. Circulation. 2005;112(4):572-577. - PubMed
-
- Tota-Maharaj R, Blaha MJ, McEvoy JW, et al. . Coronary artery calcium for the prediction of mortality in young adults <45 years old and elderly adults >75 years old. Eur Heart J. 2012;33(23):2955-2962. - PubMed
-
- Loria CM, Liu K, Lewis CE, et al. . Early adult risk factor levels and subsequent coronary artery calcification: the CARDIA Study. J Am Coll Cardiol. 2007;49(20):2013-2020. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
