

Risk factors of serious postoperative complications after pancreaticoduodenectomy and risk calculators for predicting postoperative complications: a nationwide study of 17,564 patients in Japan
- PMID: 28196308
- PMCID: PMC5516144
- DOI: 10.1002/jhbp.438
Risk factors of serious postoperative complications after pancreaticoduodenectomy and risk calculators for predicting postoperative complications: a nationwide study of 17,564 patients in Japan
Abstract
Background: The morbidity rate after pancreaticoduodenectomy remains high. The objectives of this retrospective cohort study were to clarify the risk factors associated with serious morbidity (Clavien-Dindo classification grades IV-V), and create complication risk calculators using the Japanese National Clinical Database.
Methods: Between 2011 and 2012, data from 17,564 patients who underwent pancreaticoduodenectomy at 1,311 institutions in Japan were recorded in this database. The morbidity rate and associated risk factors were analyzed.
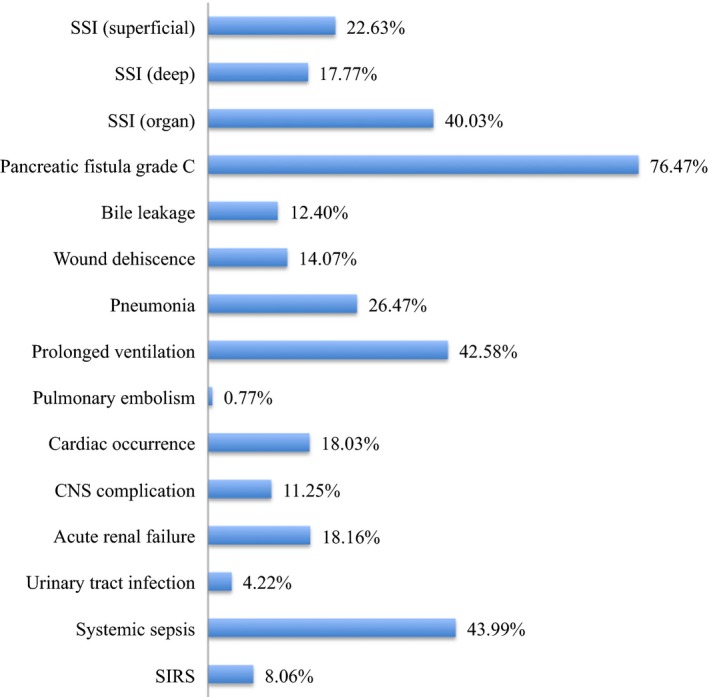
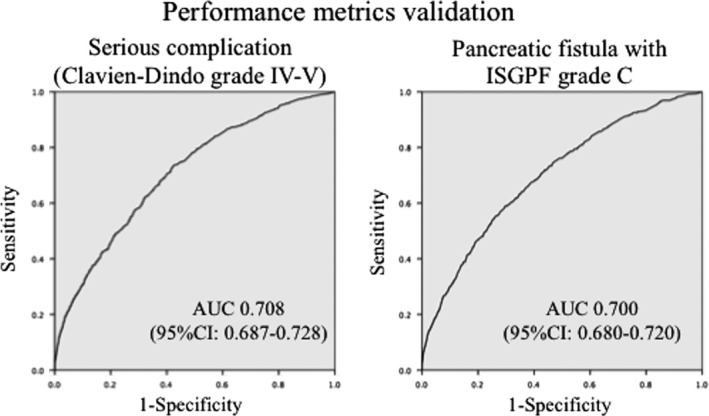
Results: The overall and serious morbidity rates were 41.6% and 4.5%, respectively. A pancreatic fistula (PF) with an International Study Group of Pancreatic Fistula (ISGPF) grade C was significantly associated with serious morbidity (P < 0.001). Twenty-one variables were considered statistically significant predictors of serious complications, and 15 of them overlapped with those of a PF with ISGPF grade C. The predictors included age, sex, obesity, functional status, smoking status, the presence of a comorbidity, non-pancreatic cancer, combined vascular resection, and several abnormal laboratory results. C-indices of the risk models for serious morbidity and grade C PF were 0.708 and 0.700, respectively.
Conclusions: Preventing a PF grade C is important for decreasing the serious morbidity rate and these risk calculations contribute to adequate patient selection.
Keywords: Pancreaticoduodenectomy; Postoperative complications; Risk calculator.
© 2017 Japanese Society of Hepato-Biliary-Pancreatic Surgery.
Figures
References
-
- Vin Y, Sima CS, Getrajdman GI, Brown KT, Covey A, Brennan MF, et al. Management and outcomes of postpancreatectomy fistula, leak, and abscess: results of 908 patients resected at a single institution between 2000 and 2005. J Am Coll Surg. 2008;207:490–8. - PubMed
-
- Winter JM, Cameron JL, Campbell KA, Arnold MA, Chang DC, Coleman J, et al. 1423 pancreaticoduodenectomies for pancreatic cancer: a single‐institution experience. J Gastrointest Surg. 2006;10:1199–210. - PubMed
-
- Schmidt CM, Powell ES, Yiannoutsos CT, Howard TJ, Wiebke EA, Wiesenauer CA, et al. Pancreaticoduodenectomy: a 20‐year experience in 516 patients. Arch Surg. 2004;139:718–25. - PubMed
-
- Behrman SW, Rush BT, Dilawari RA. A modern analysis of morbidity after pancreatic resection. Am Surg. 2004;70:675–82. - PubMed
-
- Watanabe M, Miyata H, Gotoh M, Baba H, Kimura W, Tomita N, et al. Total gastrectomy risk model: data from 20,011 Japanese patients in a nationwide internet‐based database. Ann Surg. 2014;260:1034–9. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
