

The success of pre-hospital tracheal intubation by different pre-hospital providers: a systematic literature review and meta-analysis
- PMID: 28196506
- PMCID: PMC5309978
- DOI: 10.1186/s13054-017-1603-7
The success of pre-hospital tracheal intubation by different pre-hospital providers: a systematic literature review and meta-analysis
Abstract
Background: Pre-hospital basic airway interventions can be ineffective at providing adequate oxygenation and ventilation in some severely ill or injured patients, and advanced airway interventions are then required. Controversy exists regarding the level of provider required to perform successful pre-hospital intubation. A previous meta-analysis reported pre-hospital intubation success rates of 0.849 for non-physicians versus 0.991 for physicians. The evidence base on the topic has expanded significantly in the last 10 years. This study systematically reviewed recent literature and presents comprehensive data on intubation success rates.
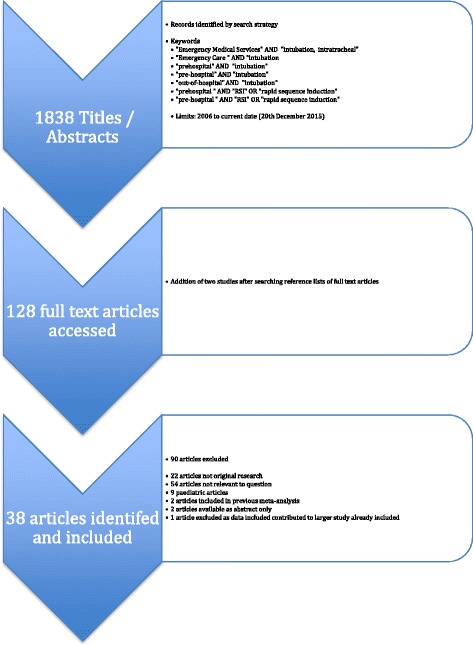
Methods: A systematic search of MEDLINE and EMBASE was performed using PRISMA methodology to identify articles on pre-hospital tracheal intubation published between 2006 and 2016. Overall success rates were estimated using random effects meta-analysis. The relationship between intubation success rate and provider type was assessed in weighted linear regression analysis.
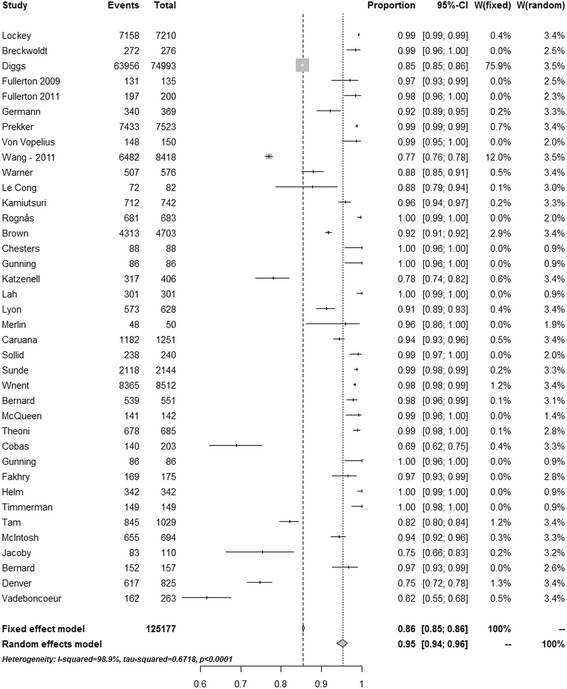
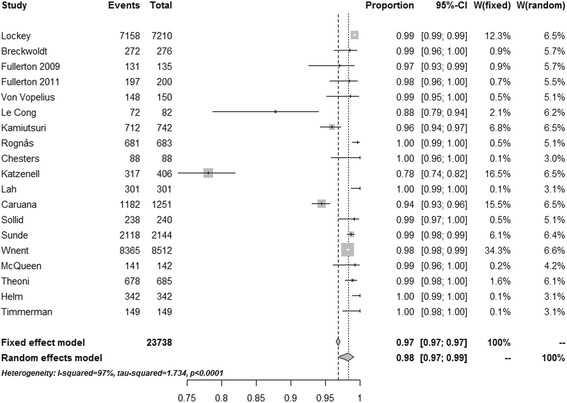
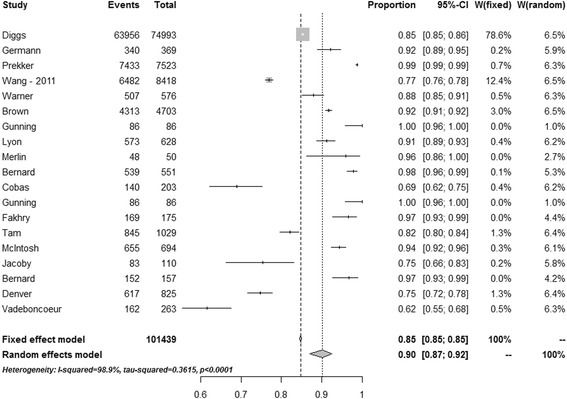
Results: Of the 1838 identified studies, 38 met the study inclusion criteria. Intubation was performed by non-physicians in half of the studies and by physicians in the other half. The crude median (range) reported overall success rate was 0.969 (0.616-1.000). In random effects meta-analysis, the estimated overall intubation success rate was 0.953 (0.938-0.965). The crude median (range) reported intubation success rates for non-physicians were 0.917 (0.616-1.000) and, for physicians, were 0.988 (0.781-1.000) (p = 0.003).
Discussion: The reported overall success rate of pre-hospital intubation has improved, yet there is still a significant difference between non-physician and physician providers. The finding that less-experienced personnel perform less well is not unexpected, but since there is considerable evidence that poorly performed intubation carries a significant risk of morbidity and mortality careful consideration should be given to the training and experience required to deliver this intervention safely.
Keywords: Airway management; Intubation; Pre-hospital emergency care; Systemic literature review.
Figures
References
-
- Jaber S, Amraoui J, Lefrant J-Y, Arich C, Cohendy R, Landreau L, et al. Clinical practice and risk factors for immediate complications of endotracheal intubation in the intensive care unit: a prospective, multiple-center study. Crit Care Med. 2006;34:2355–2361. doi: 10.1097/01.CCM.0000233879.58720.87. - DOI - PubMed
-
- Nolan JP, Soar J, Cariou A, Cronberg T, Moulaert VRM, Deakin CD, et al. European Resuscitation Council and European Society of Intensive Care Medicine Guidelines for Post-resuscitation Care 2015: Section 5 of the European Resuscitation Council Guidelines for Resuscitation 2015. Resuscitation. 2015;95:202–222. doi: 10.1016/j.resuscitation.2015.07.018. - DOI - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
