

Diabetes Control and the Risks of ESRD and Mortality in Patients With CKD
- PMID: 28196649
- PMCID: PMC5526715
- DOI: 10.1053/j.ajkd.2016.11.018
Diabetes Control and the Risks of ESRD and Mortality in Patients With CKD
Abstract
Background: Diabetes is the leading cause of end-stage renal disease (ESRD) and a significant contributor to mortality in the general population. We examined the associations of hemoglobin A1c (HbA1c) levels with ESRD and death in a population with diabetes and chronic kidney disease (CKD).
Study design: Cohort study.
Setting & participants: 6,165 patients with diabetes (treated with oral hypoglycemic agents and/or insulin) and CKD stages 1 to 5 at a large health care system.
Predictor: HbA1c level (examined as a categorical and continuous measure).
Outcomes: All-cause and cause-specific mortality ascertained from the Ohio Department of Health mortality files and ESRD ascertained from the US Renal Data System.
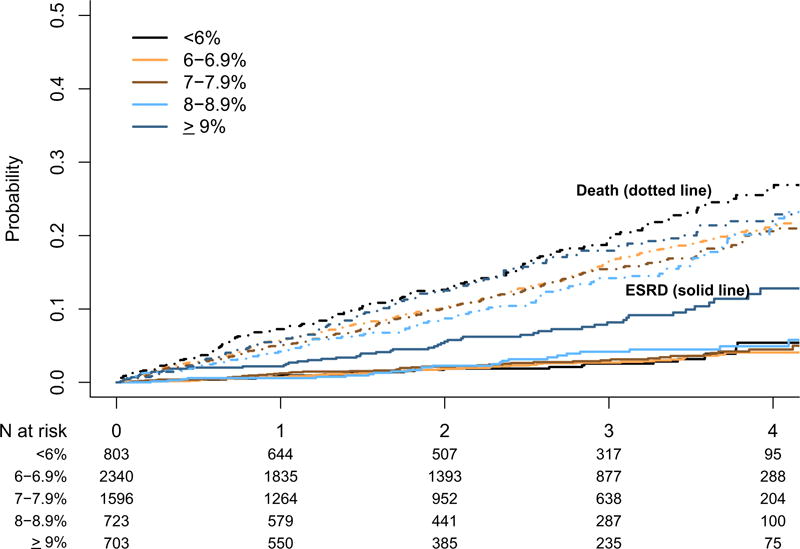
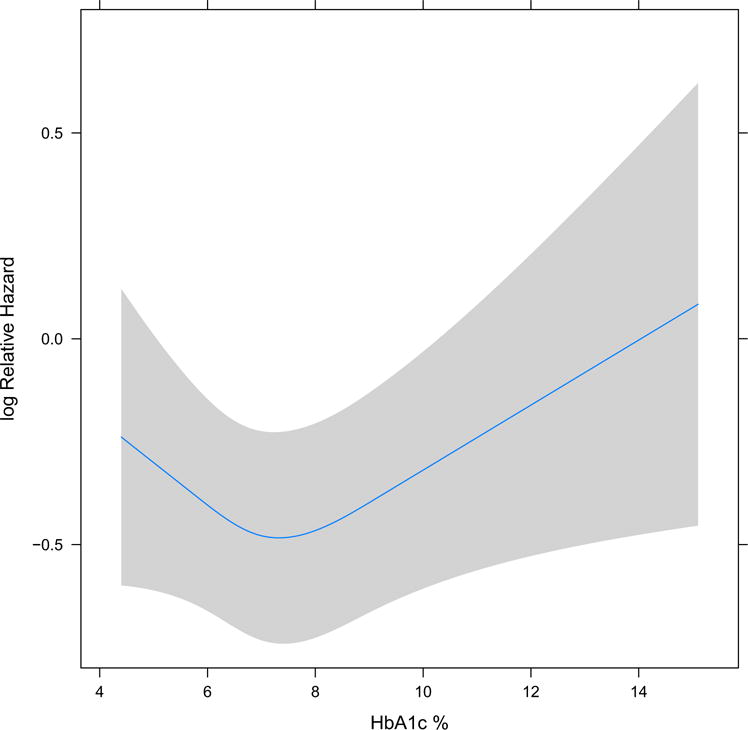
Results: During a median 2.3 years of follow-up, 957 patients died (887 pre-ESRD deaths) and 205 patients reached ESRD. In a Cox proportional hazards model, after multivariable adjustment including for kidney function, HbA1c level < 6% was associated with higher risk for death when compared with HbA1c levels of 6% to 6.9% (HR, 1.23; 95% CI, 1.01-1.50). Similarly, HbA1c level ≥ 9% was associated with higher risk for all-cause death (HR, 1.34; 95% CI, 1.06-1.69). In competing-risk models, baseline HbA1c level was not associated with ESRD. For cause-specific mortality, diabetes accounted for >12% of deaths overall and >19% of deaths among those with HbA1c levels > 9%.
Limitations: Small proportion of participants with advanced kidney disease; single-center population.
Conclusions: In this cohort of patients with CKD with diabetes, HbA1c levels < 6% and ≥9% were associated with higher risk for death. HbA1c levels were not associated with ESRD in this specific CKD population. Diabetes-related deaths increased with higher HbA1c levels.
Keywords: Glycated hemoglobin; HbA(1c); chronic kidney disease (CKD); death and kidney disease; diabetes control; diabetes mellitus; diabetic nephropathy; end stage renal disease (ESRD); incident ESRD; mortality.
Copyright © 2017 National Kidney Foundation, Inc. Published by Elsevier Inc. All rights reserved.
Conflict of interest statement
Financial Disclosure
Dr Navaneethan has served as consultant for Bayer and Boeringher-Ingelheim. The other authors declare that they have no relevant financial interests.
Figures
References
-
- Haffner SM, Lehto S, Ronnemaa T, Pyorala K, Laakso M. Mortality from coronary heart disease in subjects with type 2 diabetes and in nondiabetic subjects with and without prior myocardial infarction. N Engl J Med. 1998;339(4):229–234. - PubMed
-
- Tonelli M, Muntner P, Lloyd A, et al. Risk of coronary events in people with chronic kidney disease compared with those with diabetes: a population-level cohort study. Lancet. 2012;380(9844):807–814. - PubMed
-
- USRDS. Incidence, prevalence, patient characteristics, and treatment modalities. 2016;2016(08/04)
-
- Duckworth W, Abraira C, Moritz T, et al. Glucose control and vascular complications in veterans with type 2 diabetes. N Engl J Med. 2009;360(2):129–139. - PubMed
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
