

Impaired cardiac and skeletal muscle bioenergetics in children, adolescents, and young adults with Barth syndrome
- PMID: 28196853
- PMCID: PMC5309577
- DOI: 10.14814/phy2.13130
Impaired cardiac and skeletal muscle bioenergetics in children, adolescents, and young adults with Barth syndrome
Abstract
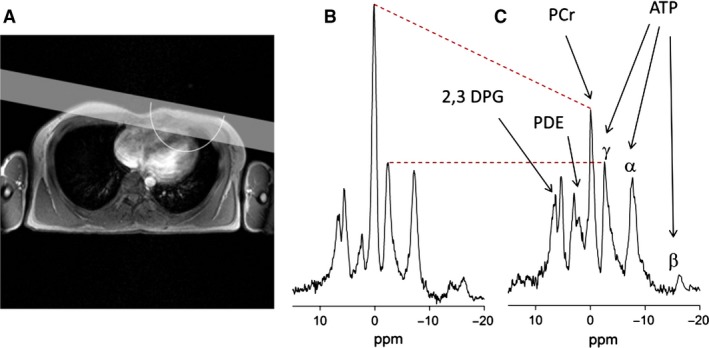
Barth syndrome (BTHS) is an X-linked condition characterized by altered cardiolipin metabolism and cardioskeletal myopathy. We sought to compare cardiac and skeletal muscle bioenergetics in children, adolescents, and young adults with BTHS and unaffected controls and examine their relationships with cardiac function and exercise capacity. Children/adolescents and young adults with BTHS (n = 20) and children/adolescent and young adult control participants (n = 23, total n = 43) underwent 31P magnetic resonance spectroscopy (31P-MRS) of the lower extremity (calf) and heart for estimation of skeletal muscle and cardiac bioenergetics. Peak exercise testing (VO2peak) and resting echocardiography were also performed on all participants. Cardiac PCr/ATP ratio was significantly lower in children/adolescents (BTHS: 1.5 ± 0.2 vs.
Control: 2.0 ± 0.3, P < 0.01) and adults (BTHS: 1.9 ± 0.2 vs.
Control: 2.3 ± 0.2, P < 0.01) with BTHS compared to Control groups. Adults (BTHS: 76.4 ± 31.6 vs.
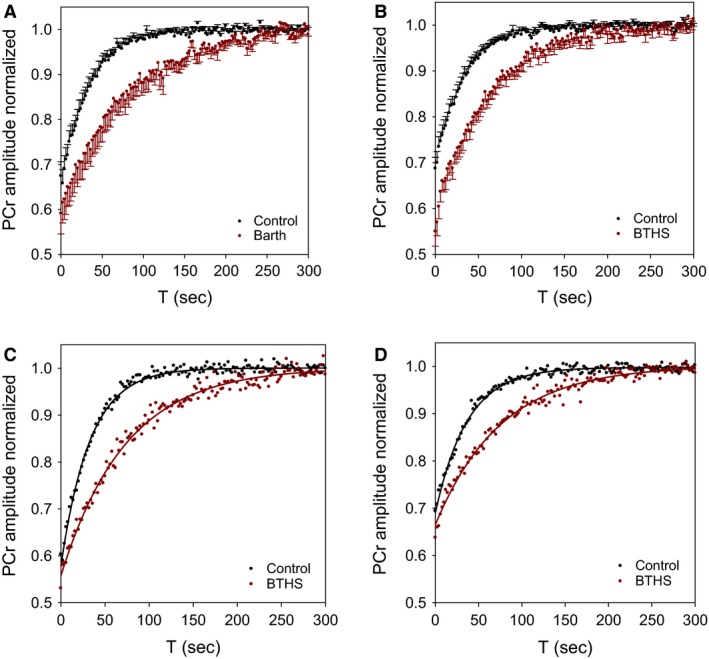
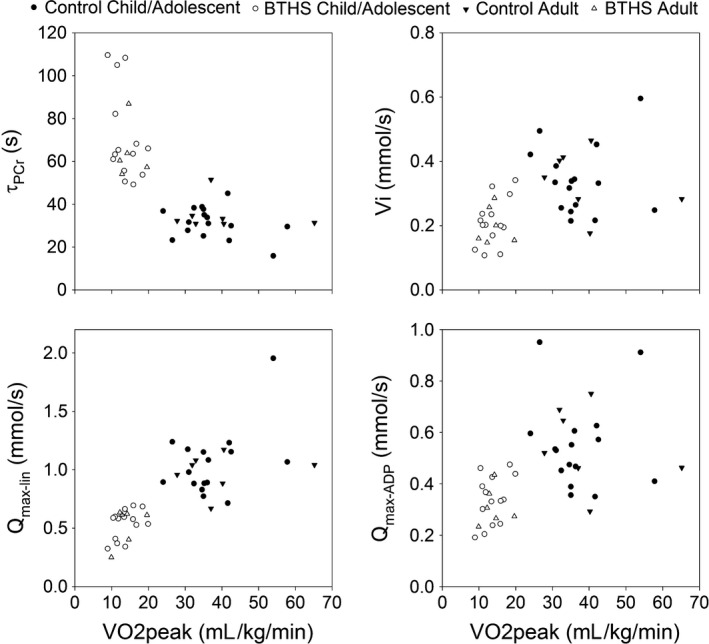
Control: 35.0 ± 7.4 sec, P < 0.01) and children/adolescents (BTHS: 71.5 ± 21.3 vs.
Control: 31.4 ± 7.4 sec, P < 0.01) with BTHS had significantly longer calf PCr recovery (τPCr) postexercise compared to controls. Maximal calf ATP production through oxidative phosphorylation (Qmax-lin) was significantly lower in children/adolescents (BTHS: 0.5 ± 0.1 vs.
Control: 1.1 ± 0.3 mmol/L per sec, P < 0.01) and adults (BTHS: 0.5 ± 0.2 vs.
Control: 1.0 ± 0.2 mmol/L sec, P < 0.01) with BTHS compared to controls. Blunted cardiac and skeletal muscle bioenergetics were associated with lower VO2peak but not resting cardiac function. Cardiac and skeletal muscle bioenergetics are impaired and appear to contribute to exercise intolerance in BTHS.
Keywords: Barth syndrome; energetics; exercise; mitochondria; muscle.
© 2017 The Authors. Physiological Reports published by Wiley Periodicals, Inc. on behalf of The Physiological Society and the American Physiological Society.
Figures
References
-
- Altschuld, R. A. , and Brierley G. P.. 1977. Interaction between the creatine kinase of heart mitochondria and oxidative phosphorylation. J. Mol. Cell. Cardiol. 9:875–896. - PubMed
-
- American College of Sports Medicine . 2000. ACSM's guidelines for exercise testing and prescription. Lippincott, Williams & Wilkins, Baltimore.
-
- Bahi, L. , Koulmann N., Sanchez H., Momken I., Veksler V., Bigard A. X., et al. 2004. Does ACE inhibition enhance endurance performance and muscle energy metabolism in rats? J. Appl. Physiol. (1985) 96:59–64. - PubMed
-
- Barth, P. G. , Scholte H. R., Berden J. A., derVan Klei‐Van Moorsel J. M. , Luyt‐Houwen I. E., Van ‘t Veer‐Korthof E. T., et al. 1983. An X‐linked mitochondrial disease affecting cardiac muscle, skeletal muscle and neutrophil leucocytes. J. Neurol. Sci. 62: 327–355. - PubMed
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
