

Outcome of Noncardiac Surgical Patients Admitted to a Multidisciplinary Intensive Care Unit
- PMID: 28197046
- PMCID: PMC5278585
- DOI: 10.4103/0972-5229.198321
Outcome of Noncardiac Surgical Patients Admitted to a Multidisciplinary Intensive Care Unit
Abstract
Context: Surgical procedures carry significant morbidity and mortality depending on the type of surgery and patients. There is a dearth of evidence from India on the outcome of surgical patients admitted to an Intensive Care Unit (ICU).
Aims: We aimed to describe the incidence and risk factors of postoperative complications and mortality in noncardiac surgical patients admitted to the ICU.
Settings and design: This was a prospective observational study on all perioperative patients admitted to a multidisciplinary ICU for 18 months.
Subjects and methods: Data on demography, admission Acute Physiology and Chronic Health Evaluation II (APACHE-II), Sequential Organ Failure Assessment (SOFA) scores, perioperative course, type and duration of surgery, reason for ICU admission, ICU interventions, and perioperative complications were recorded. The primary outcomes analyzed were perioperative complications and mortality.
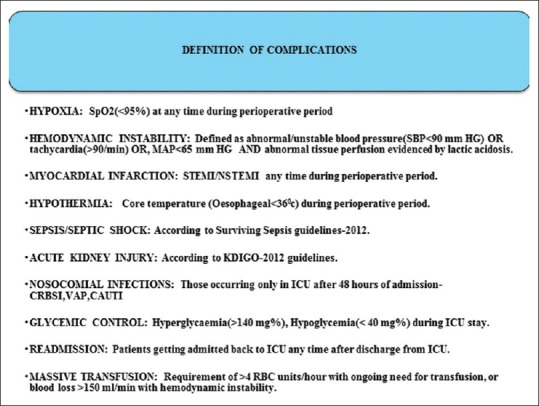
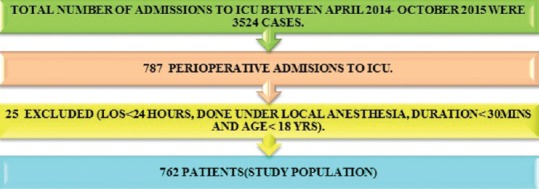
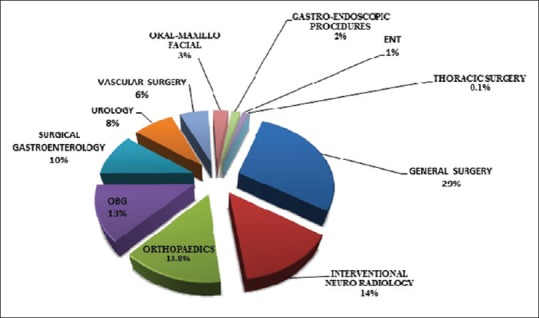
Results: The study included 762 patients with a mean age of (mean ± standard deviation [SD]) 50.5 ± 18 years and a male (58.4%) preponderance. The mean (±SD) admission APACHE-II and SOFA scores were 15 (±5.0) and 4.26 (±2.6), respectively. The most common reason for ICU admission was elective mechanical ventilation 50%, followed by prolonged surgery 26.2% and hemodynamic instability 21.2%. Most (51.1%) patients belonged to American Society of Anaesthesiologists physical Status III or IV and Lee's surgical risk Category I and II (66.8%). The most common surgical procedures performed were gastro-intestinal (28.5%) followed by interventional Neuro-radiology (14.0%) and orthopedic (13.9%). Overall perioperative complications were observed in 51.4% (n = 392). Common complications observed were hemodynamic instability 24%, hypothermia 17.2%, sepsis 17.3%, poor glycemic control 11.2%, perioperative myocardial infarction 7.1%, cardiac arrest 0.13%, and acute kidney injury (AKI) 10.1%. The overall hospital mortality was 7.9%. Multivariate logistic regression analysis showed that admission APACHE-II score, sepsis, AKI, and ICU length of stay were independent predictors for mortality.
Conclusions: High risk perioperative patients after noncardiac surgery have significant mortality and morbidity.
Keywords: Critically ill; noncardiac surgical patients; perioperative patients.
Conflict of interest statement
There are no conflicts of interest.
Figures
References
-
- Pearse RM. Another inconvenient truth: Meeting the challenge of preventing poor surgical outcomes. Curr Opin Crit Care. 2010;16:337–8. - PubMed
-
- Jhanji S, Pearse RM. The use of early intervention to prevent postoperative complications. Curr Opin Crit Care. 2009;15:349–54. - PubMed
-
- Moonesinghe SR, Mythen MG, Grocott MP. High-risk surgery: Epidemiology and outcomes. Anesth Analg. 2011;112:891–901. - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources